
Mission
Arogya World works to prevent noncommunicable diseases (NDCs) in India through health education and lifestyle change, leveraging technology and partnerships to help people lead healthier lives. It accomplishes this through an innovative, community-based doorstep health model, delivering prevention programming outside of traditional healthcare systems to reach people where they live, learn, and work.
Life Challenges of the Women Served
 The Noncommunicable Disease (NCD) crisis in India is one of the most significant health and development challenges of the century. The current incidence of NCD in India is staggering:
The Noncommunicable Disease (NCD) crisis in India is one of the most significant health and development challenges of the century. The current incidence of NCD in India is staggering:
- NCDs account for nearly two-thirds of deaths.
- 77 million have diabetes and an equal number are estimated to be prediabetic.
- 75 percent of adults in metros like Delhi and Chennai are diabetic or prediabetic.
- 20 percent have a chronic disease.
- 10 percent have more than one chronic disease.
- One in three adults has high blood pressure.
- South Asians account for 60 percent of the world’s heart patients.
The burden of NCDs is far-reaching and affects individuals, families, and all socio-economic levels and facets of society. NCDs cause a financial burden for individuals and families due to the high cost of treatment and the loss of stable employment. This is especially true in vulnerable communities where the cost of healthcare is out of reach and therefore, the financial consequences are catastrophic. For instance, 25 percent of a poor family’s income is spent on one diabetic family member, which is why many families borrow money from friends or family to pay for it. Add to that the healthcare costs associated with complications of diabetes and hospitalizations – heart disease, stroke, kidney disease and dialysis, nerve damage and foot amputation, and blindness – and the toll of NCDs from a human suffering and cost perspective is alarming.
The economic impact of NCDs on society is also devastating and will continue to grow. India is a young country with 50 percent of the population under age 25. With Indians getting diabetes in their 30s and 40s (10 years earlier than Westerners), and while at the peak of their productive years, the potential negative impact on the country’s economy is a serious concern. India stands to incur a loss of $4.58 trillion in economic output by 2030 due to NCDs. The recent pandemic and the close links between diabetes and COVID will be debilitating for India’s already overburdened and fragile healthcare system.
 The NCD crisis greatly impacts one of the largest segments of India’s population: adolescents. Young people in India account for every fifth person or 280 million people. Adolescence is a nutritionally vulnerable time when rapid physical growth increases nutrient demands. Adolescents experience a triple burden of malnutrition: undernutrition, overweight, and hidden hunger caused by a lack of essential nutrients. The incidence of overweight and obesity is increasing, more than 10 percent of those ages 10 to 19 are prediabetic, and the rate of childhood diabetes has increased three-fold over the last 30 years. Unhealthy diet, physical inactivity (75 percent of Indian children get insufficient physical activity), and tobacco use make young people prone to NCDs at an early age, including cardiovascular diseases (CVDs), cancer, and diabetes.
The NCD crisis greatly impacts one of the largest segments of India’s population: adolescents. Young people in India account for every fifth person or 280 million people. Adolescence is a nutritionally vulnerable time when rapid physical growth increases nutrient demands. Adolescents experience a triple burden of malnutrition: undernutrition, overweight, and hidden hunger caused by a lack of essential nutrients. The incidence of overweight and obesity is increasing, more than 10 percent of those ages 10 to 19 are prediabetic, and the rate of childhood diabetes has increased three-fold over the last 30 years. Unhealthy diet, physical inactivity (75 percent of Indian children get insufficient physical activity), and tobacco use make young people prone to NCDs at an early age, including cardiovascular diseases (CVDs), cancer, and diabetes.
Rural communities, which account for two-thirds of the population in India, are also greatly impacted by NCDs because of their decreased access to healthcare and resources, including prevention education. Rural Indian adolescent girls are especially impacted and are hard hit with this triple burden of malnutrition. They show evidence of stunting, very high anemia (59 percent of females ages 15 to 19 are anemic), vitamin A and D deficiency, high dropout rates from school, and early marriage before age 18. Being malnourished themselves, they have low birthweight babies, continuing the intergenerational cycle of poverty and NCDs.
The story of diabetes in Indians is complex and evolving. India’s rapid urbanization and accompanying modern lifestyle changes, including decreased physical activity and higher consumption of convenience foods, junk food, sugary drinks, and overall calories, are major contributing factors to elevated diabetes rates in India. The aggressive marketing practices of Big Food and Big Tobacco and the inadequate healthcare system are also systemic causes. In addition, there is evidence that Indians have a greater degree of insulin resistance and a stronger genetic predisposition to diabetes. Furthermore, the low birthweight of babies born to undernourished young mothers is another factor for high rates of heart disease and diabetes in the children when they grow up.

According to the World Health Organization, NCDs are largely preventable. Eighty percent of diabetes and 80 percent of heart disease can be prevented with three lifestyle changes: eating right, exercising, and avoiding tobacco. While these simple preventive care practices are extremely effective in avoiding NCDs, lack of awareness combined with poor adoption of positive behaviors creates a critical gap. Exposure to risk factors begins in childhood and builds throughout life. Thus, it is critical to enable positive behavior changes toward healthy living by carefully engaging with people at an individual and community level. However, overburdened health workers in overcrowded health facilities are unable to take out the time to provide information and counsel on adoption of healthy behaviors.
The Project
Arogya World (AW) seeks to improve the nutritional status and healthy behaviors in rural adolescent girls. Participating girls improve their eating habits and physical activity levels and ultimately reduce their risk of NCDs. They also learn the value of avoiding tobacco and gain an appreciation for healthy living. The goal is to increase the adoption of these healthy behaviors by 15 percent. Research confirms that improved health leads to increased productivity and ultimately, a reduction in poverty due to fewer health-related work interruptions, increased stability, and heightened upward mobility. Thus, this program will have a tremendous impact on the girls’ futures. With this solid grounding in health at an early age, they will have more opportunities to participate in the workforce and become more financially self-sufficient. Additionally, AW’s activities reinforce leadership skills and improve girls’ confidence, further supporting their future career opportunities and ability to be self-sufficient. They will also be able to steer their current families and the future families towards healthy living.
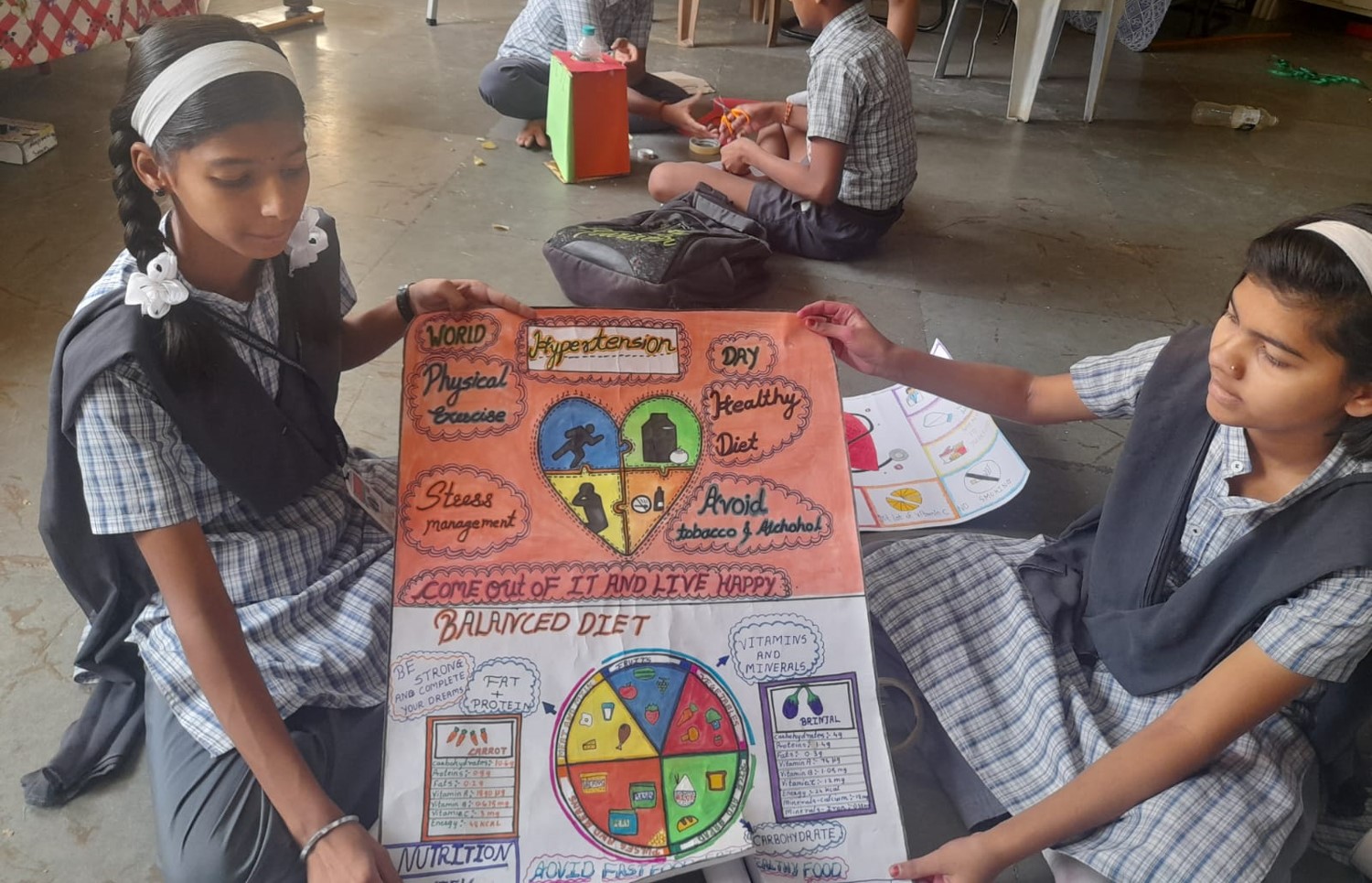
This project takes place in Gujarat, India. It will test the effectiveness and impact of Rural MyThali, which translates India’s National Institute of Nutrition (NIN) guidelines into an easy-to-follow picture format that is region-specific. This will be integrated into Arogya World’s Healthy Schools health education program, which has been proven to work and has been deployed in 500,000 children around the country. In 2020, India’s top nutrition experts requested that AW integrate MyThali into the existing program and deliver it to large numbers of girls in school, but the work was delayed by the pandemic. This project will be the first opportunity to develop a formal integrated program for a nutrition tool in the school setting and test its effectiveness in adolescent girls, who most often are forgotten in the design of nutrition programs.
AW’s health education for adolescents aligns with best practices and guidelines set by the government. Schools have been identified as ideal platforms to facilitate healthy behaviors in children and adolescents, and to mobilize parents and communities around health. Studies also indicate that adolescents should be prioritized as target groups for interventions due to their high adaptability and likelihood to be motivated for appropriate lifestyle modifications, and the fact that most of the NCD risk factors are behaviorally acquired during adolescence. Thus, educating adolescents about the basics of healthy living before their lifestyle habits are set is a smart solution to the NCD crisis. In addition, by incorporating feedback directly from the communities and program recipients, AW will be able to customize the program to be relevant and accessible to the target population, which is a best practice for any behavior change intervention.
The project unfolds in four phases:
Phase 1: Formative Research – By administering questionnaires to the girls, measuring health metrics, and gathering information from district authorities, data will be collected in participants including:
- Socio-demographic profile of school-going girls
- Anthropometry-based nutritional status and anemia prevalence and morbidity profile (15-day reference period)
- Assessment of knowledge about basic aspects of foods, nutrition and anemia
- Dietary practices and dietary diversity
- Information on interventions under various national or local programs and girls’ utilization of these services
Phase 2: Development of Action Plan / MyThali activity calendar for 12 weeks – To support the use of MyThali comic book on basics of Foods and Nutrition, additional region-specific, culturally relevant tools will be developed, including:
- Counseling cards
- Traditional Indian “Toran” (similar to a garland) depicting the My Thali concept to be placed in
- strategic places at the school
- Activities such as rally, quiz, Snakes and Ladders game, and board games
- The integrated MyThali + Healthy Schools program

Phase 3: Capacity building – Development and pretesting of intervention Tool Kit in vernacular language using regional meals
- The Tool Kit will be used to implement the current project and will also be left behind so the schools can continue to use it in future years for fresh incoming seventh grade girls
- Two peer-educators will be identified per school
- Training of all implementers
- Activities will be implemented by the peer-educators and completed on time – the program will be provided to all students in the designated classroom (both boys and girls)
- Sessions conducted by peer educators will be monitored through spot checking and observation checklist by designated monitors.
Phase 4: Impact Evaluation: The impact of the Healthy Schools + Rural MyThali intervention on the adolescent girls will be assessed based on knowledge, attitudes and behaviors including on physical activity, dietary practices, nutritional status, hemoglobin levels, dietary diversity and morbidity profile. Data collection will be done on the phones of field staff using a questionnaire adapted from Arogya World’s existing questionnaires. Hemoglobin levels for the girls (a subset) will be measured in the local primary health center. All these measurements will be carried out at two timepoints – baseline (before the start of the intervention) and endline (when the intervention ends).
 This project will directly reach 1,600 seventh grade girls in Gujarat in year one and an equal number in year two. Each year, 8,000 family members will benefit indirectly. One in four girls in the state get married before the legal age and only 48 percent of women are literate compared to the national rate of 70 percent. Eight hundred of these girls (400 participants and 400 controls) will be from the Aspirational District of Narmada. This district is designated by the Indian Government as aspirational because of its severe underdevelopment and high poverty rates. Thirty-seven percent of the population in Narmada is considered multidimensionally poor based on health, education, and standard of living indicators.
This project will directly reach 1,600 seventh grade girls in Gujarat in year one and an equal number in year two. Each year, 8,000 family members will benefit indirectly. One in four girls in the state get married before the legal age and only 48 percent of women are literate compared to the national rate of 70 percent. Eight hundred of these girls (400 participants and 400 controls) will be from the Aspirational District of Narmada. This district is designated by the Indian Government as aspirational because of its severe underdevelopment and high poverty rates. Thirty-seven percent of the population in Narmada is considered multidimensionally poor based on health, education, and standard of living indicators.
An additional 800 girls from rural village communities surrounding Baroda will be included in the project, with 400 receiving the intervention and 400 acting as the control group. Adolescent girls in this region are also exceedingly vulnerable to reduced access to education, premature marriage, and prevailing patriarchal norms of gender inequality. In addition, these rural regions in Gujarat have poorer health indicators compared to urban areas.
AW will implement the program for boys and girls but will collect and report data only for girls.
This project’s reach will extend far beyond the direct beneficiaries to include various additional groups including the girls’ current and future households, boys in the intervention classrooms, friends and other community members, and future waves of students.
A key component of this project is co-developing the programming and materials along with the targeted women and girls. AW will implement focus groups with the girls and their mothers to understand food preferences/habits along with locally available food and to assess their knowledge and perception of different foods, nutrition, and anemia. Additionally, AW will work closely with participants to understand common food habits and dietary patterns in the area in order to better tailor the curriculum and materials to be relevant and accessible for girls in the region. AW will also rely on peer educators from the villages in which they are working to deliver the content. These girls will be true peers of the girls they are teaching and can bring their shared experience and perspectives into the program they are delivering.
Year 1 – Direct Impact: 1,600 (800 intervention); Indirect Impact: approximately 8,000 family members
Year 2 – Direct Impact: 1,600 (800 intervention); Indirect Impact: approximately 8,000 family members
UN Sustainable Development Goals
![]()
Questions for Discussion
- Why is delivering programming where people “live, learn, and work” more effective than traditional methods?
- How do you think a reduction in NCDs can affect gender equality?
- What roadblocks might a girl experience when trying to introduce nutrition, exercise, and anti-tobacco changes to her family?
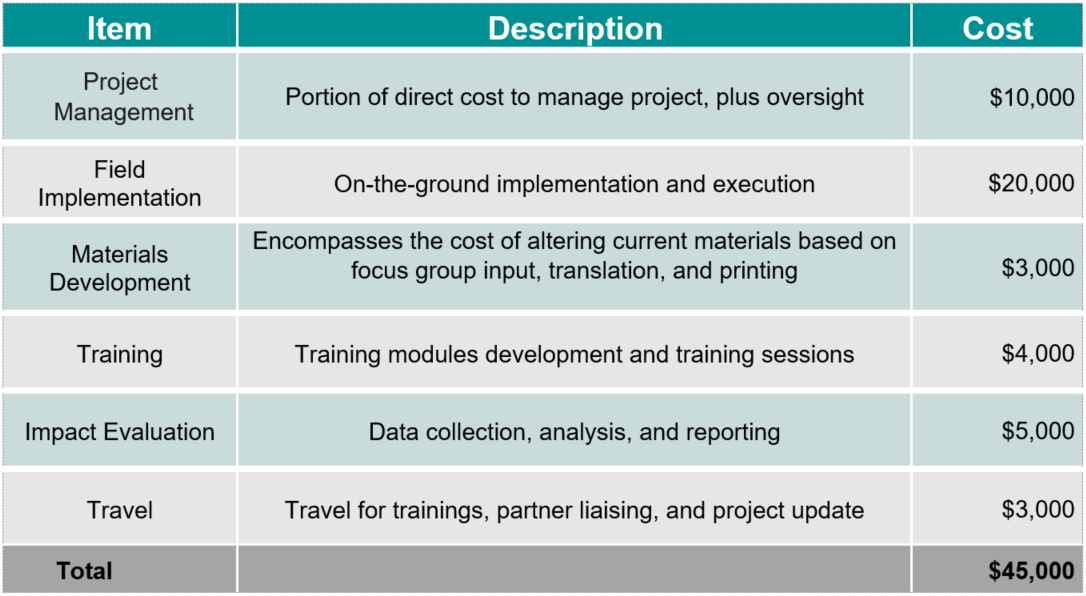
How the Grant Will be Used
Together Women Rise’s grant of $45,000 over two years will help fund the following:
Why We Love This Project/Organization
We love that this is a science-based diabetes and other non-communicable disease (NCD) program. It adds a nutrition and diet component to a health program in school. It focuses on adolescent girls – a key stage in the lifecycle of nutritional poverty. It is sustainable because the toolkit will be available in schools after the intervention. And it offers the opportunity to educate about the different “faces” of poor nutrition, which can include over-nutrition and obesity.
Evidence of Success
Arogya World has been recognized for its tremendous work in global health through the receipt of several awards, including:
- 2022 UN Interagency Task Force and the WHO Special Program on Primary Health Care Award – recognized Arogya World for its work in scaling up community-based delivery models to strengthen the prevention and control of diabetes at the population level across 19 states in India
- mBillionth Award for mDiabetes (2013)
- Finalist – Drucker Institute Award for Nonprofit Innovation (2013)
- Nalini Saligram (founding board member) recognized as an Ashoka Fellow (2015)
- Featured in The Healthcare Gamechangers book by Dr. Ashwin Naik (2019)
- Google AI for Social Good (2021)
- Made and fulfilled several Clinton Global Initiative Commitments
Arogya World’s programs have demonstrated impact on improving knowledge and adoption of healthy behaviors. The program uses a monitoring and evaluation framework supported by strong partnerships and a digital backbone for data collection and analysis.

Voices of the Girls
“Before when I used to check the lunch boxes of all my friends in class, they used to get lot of junk and unhealthy food. After the awareness program by Hriday & Arogya World, they have started getting healthy foods for lunch.” – Peer Leader of Arogya Healthy, Schools Program, Delhi.
“These diseases have affected us badly because they (my parents) are sick, and there’s no money… the truth is I’m tired…but I have to take care of them.” – A woman who cares for her parents who suffer from NCDs
“I study in KGVB, Kadambu, RES, Bagalkot. Today people from Arogya World and Agastya Foundation came to our school to teach us about diabetes awareness and prevention. This workshop was very informative and we could later spread this useful information to our family members. For this, I would like to thank Arogya World and Agastya Foundation on behalf of my school and me.” – Student from the Healthy Schools Program
“Because of Arogya, we have discussed in the teacher-student meeting and made lot of changes in our cafeteria in terms of offering healthy options: vegetable sandwiches, fruit chat, nimbu pani, etc., instead of cool drinks, and less of oil, and no junk-packed foods at all.” – School Leader
“My child used to share what happened to her at school. She used to tell us things that we didn’t know anything about earlier. Before this the problem was that she used to fall sick often. But after she told us about the school health program, we started following it. We are healthy now, and our child is healthy too.” – Mother of Poonam, a Healthy Schools Program Participant
About the Organization
 Arogya World was established in 2010 by Dr. Nalini Saligram and three other founding board members, a group of dedicated, passionate women who had the shared goal of making an impact on global health. In 2012, Arogya World India Trust was established to further advance AW’s work in India. The two entities work in close partnership to deliver AW’s programs across India.
Arogya World was established in 2010 by Dr. Nalini Saligram and three other founding board members, a group of dedicated, passionate women who had the shared goal of making an impact on global health. In 2012, Arogya World India Trust was established to further advance AW’s work in India. The two entities work in close partnership to deliver AW’s programs across India.
AW leverages strategic partnerships, existing networks, and technology for cost-effective and impactful programs that include:
- mDiabetes, a diabetes prevention program that sends preventive care messages directly to phones of users
- Healthy Schools, which teaches adolescents the basics of healthy living through age-appropriate games and activities
- Healthy Workplaces, which assesses and supports companies on doing more for the physical and mental health of employees, and
- MyThali, which builds awareness on healthy eating and nutrition.
AW has educated 6 million people on healthy living since its inception and aims to reach 50 million in the next five years. Its programs are evidence-based, user-centered, and have demonstrated impact.
Arogya World’s work benefits diverse groups of Indians, including adolescents and adults, women, and men, from a variety of backgrounds and socioeconomic levels. The target population is program-specific: mDiabetes targets adults, many of whom are underserved, lower-income individuals, Healthy Schools focuses on adolescents ages 11-14, Healthy Workplaces targets working adults, and MyThali is directed to urban women. While their programs have a broad reach, the focus of most of the programming is on underserved, vulnerable communities as they face the greatest challenges from NCDs and have the least access to healthcare and trusted health information. This includes rural communities and in some cases the least developed aspirational districts, children studying in government schools, low-income families, and women and girls.
AW is estimated to have reached more than a million people who live on less than $5.50 a day.
Where They Work

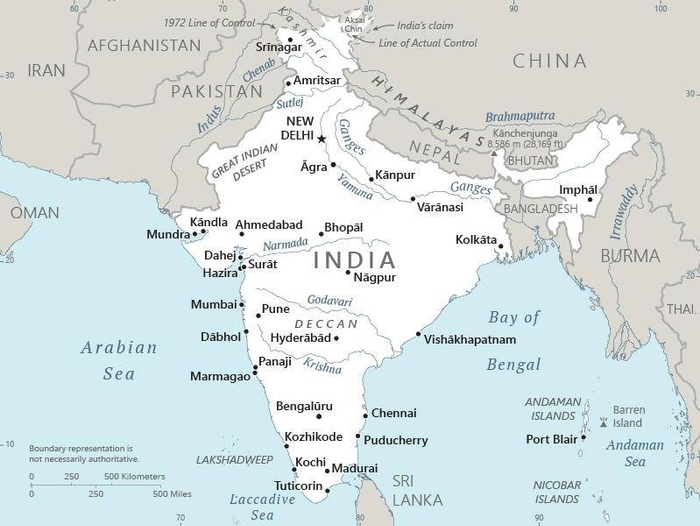
With a population of almost 1.4 billion, India is the second most populated country on Earth and the largest South Asian economy, comprising a third of Asia and over 17 percent of humanity. English is the language of choice for political and commercial endeavors, although there are 22 other recognized languages, including Hindi, which is spoken by 44 percent. Unfortunately, 360 million Indians – more than every US man, woman, and child – live in squalid conditions and are among the most impoverished in the world.
India’s slums are home to millions, yet a third are not even recognized by the government. Families crowd together in makeshift structures, drink scant and contaminated water, scrounge through waste dumps, and typically share unhygienic communal bathrooms that lack sewage systems. Twenty percent live far below the poverty line, often as domestic workers, daily wager laborers, rickshaw pullers, and other low-paying jobs. Discrimination against women and girls is rampant, corruption is entrenched, and there is an unequal distribution of quality education.
Gujarat is on the west coast of India, bordered by Pakistan and other Indian states. It is about the size of Kansas but is home to 71.5 million people versus 2.92 million in Kansas. Gujarat has the longest coastline of any Indian state. The official languages are Gujarati and Hindi. This area is among the most industrialized in India, including chemicals, dairy, pharmaceuticals, cement, ceramics, gems, jewelry, and engineering. Gujarat is also one of the world’s biggest producers of processed diamonds. Seventy-two percent of the world’s processed diamonds and 80 percent of India’s diamond exports come from Gujarat.
A closer look at NCDs in low income countries
Low income countries around the world are experiencing a rapid and relentless increase in the number of Noncommunicable Diseases (NCDs). These include cancer, mental illness, diabetes, and chronic respiratory disorders, with cardiovascular disease the primary contributor to the increase. In lower-middle income countries, NCDs make up over half the total incidence of disease, and they increasingly strike people at a younger age than in wealthier countries. This places a profound burden on all aspects of society, from individuals suffering from these diseases to their families whose personal and economic lives are upended.
Much of the health effort in low income areas has been focused on infectious diseases and improving child and maternal health. As a result, they have underdeveloped healthcare systems for NCDs and little attention is paid to prevention and chronic disease management. In many respects, people in low income countries are facing the same unhealthy hurdles faced by Americans: a proliferation of (cheap) junk food and occupations that encourage sitting all day long.
Globally, NCDs are the leading causes of death and disability. Unfortunately, NCDs both cause and exacerbate poverty. NCDs also reduce economic vitality and development in low- and middle-income countries.
Source Materials
https://impact.economist.com/perspectives/sites/default/files/The_next_pandemic.pdf
https://www.kff.org/global-health-policy/fact-sheet/the-u-s-government-and-global-non-communicable-diseases/
https://www.wonders-of-the-world.net/Taj-Mahal/India/Gujarat.php
https://www.eyeonasia.gov.sg/india/know/selected-india-states/gujarat-profile/
https://www.populationu.com/in/gujarat-population#:~:text=Gujarat%20population%20in%202023%20is,%2C%20updated%2031%2C%20March%202022
https://www.cia.gov/the-world-factbook/countries/india/summaries/#people-and-society
https://topyaps.com/n-heartbreaking-facts-about-life-in-indian-slums/
https://www.ibef.org/states/west-bengal.aspx