
Mission
CureCervicalCancer is dedicated to the early detection and prevention of cervical cancer around the globe for the women who need it most.
Life Challenges of the Women Served
Cervical cancer claims the lives of over 300,000 women every year. According to the World Health Organization (WHO), a woman dies of cervical cancer every two minutes, making it one of the greatest threats to women’s health. A disproportionate 90 percent of these women live in resource poor countries where lack of wide-scale screening fails to identify cervical cancer until it is invasive, and access to treatment for invasive cancer is extremely limited. Cervical cancer, largely, is a disease of inequality.
 Without the intervention of early detection and treatment, women in resource poor regions will continue to die from cervical cancer at an alarming rate. In fact, the WHO predicts that by 2040 cervical cancer deaths will increase by 50 percent. The world’s most vulnerable women are unjustly dying from a disease that is preventable.
Without the intervention of early detection and treatment, women in resource poor regions will continue to die from cervical cancer at an alarming rate. In fact, the WHO predicts that by 2040 cervical cancer deaths will increase by 50 percent. The world’s most vulnerable women are unjustly dying from a disease that is preventable.
With early detection and prevention, cervical cancer is nearly 100 percent preventable, yet every day it claims the lives of eight women in Kenya. These women lack access to the most basic screening and treatment services, and often seek healthcare only once the cancer has become symptomatic and fatally invasive. Women, who are the backbone of their families and their communities, are dying unnecessarily from a disease that can be easily prevented. And when a mother dies, her children are ten times less likely to survive childhood.
Cervical cancer is most frequently diagnosed between the ages of 35-44 when women are at the prime of their lives. The options for treating invasive cancer in Kenya are extremely limited and prohibitively expensive. Screening can save a woman’s life by detecting cervical cancer in the early stages when it can be easily treated. According to data, less than 13 percent of the Kenyan population has been screened for cervical cancer, largely due to lack of access and awareness.
 There is a lack of any wide-scale organized screening and treatment initiative in Kisumu, Kenya. Healthcare facilities lack the tools, infrastructure, resources, and trained personnel to provide cervical cancer screening and treatment. Women lack the awareness of the life- saving necessity of screening, and they attach stigma and fear to screening since cervical cancer is both a terminal disease and caused by a sexually transmitted virus.
There is a lack of any wide-scale organized screening and treatment initiative in Kisumu, Kenya. Healthcare facilities lack the tools, infrastructure, resources, and trained personnel to provide cervical cancer screening and treatment. Women lack the awareness of the life- saving necessity of screening, and they attach stigma and fear to screening since cervical cancer is both a terminal disease and caused by a sexually transmitted virus.
Cervical cancer usually develops without displaying symptoms until the disease is invasive and advanced. If pre-cancerous changes on the cervix are detected and treated early, a woman will not develop cervical cancer. Wide-scale screening with cervical cytology (or PAP smear) is not feasible in resource-poor countries due to lack of infrastructure and high cost. Instead, the WHO recommends a simple and cost-effective screening procedure called visual inspection with acetic acid (VIA).
The Project
CureCervicalCancer will reduce the incidence of cervical cancer in Kisumu, Kenya, by training healthcare professionals, screening and treating women, and establishing 11 permanent “See & Treat” clinics and one mobile clinic. “See & Treat” is CCC’s term for VIA, the simple and effective cervical cancer screening method recommended by WHO. With this method, pre-cancerous cervical changes can be spotted with the naked eye and the cells can be immediately treated with ablation methods of cryotherapy or thermocoagulation. This destroys the pre-cancerous tissue completely in 85 – 90 percent of cases, thereby preventing the progression to cervical cancer – and preventing needless deaths of thousands of underserved women. The program also strengthens the system of community education, patient navigation, follow-up, and referral.
 CCC’s current “See & Treat” project in Kisumu, Kenya, has resulted in 6,083 women screened and 206 treated since May 2018. DFW’s one-year grant allows CCC to significantly expand the program so that 12,160 women will be screened and 25,000 will be indirectly served by gaining an education. CCC plans to continue the project for 3-5 years to ensure the sites can permanently provide “See & Treat” services.
CCC’s current “See & Treat” project in Kisumu, Kenya, has resulted in 6,083 women screened and 206 treated since May 2018. DFW’s one-year grant allows CCC to significantly expand the program so that 12,160 women will be screened and 25,000 will be indirectly served by gaining an education. CCC plans to continue the project for 3-5 years to ensure the sites can permanently provide “See & Treat” services.
This project targets Kenyan women between the ages of 18-49 who have never been screened for cervical cancer. These women are medically underserved and socioeconomically disadvantaged. Participants include indigenous peoples, female prisoners, sex workers, LGBTQ, refugees, and women with HIV. (HIV-positive women are five times more likely to contract cervical cancer due to a compromised immune system.) Recognizing that men often make healthcare decisions for the women in their family, this project will also target men through community education and awareness.
Expansion of CCC’s program entails key steps and activities that address the existing impediments:
- Testing Centers: CCC will offer testing at 11 healthcare facilities and one mobile clinic to actively provide screening and treatment. These testing centers will serve 12,160 women and treat 100 percent of the positive screens.
- Training & Mentorship: CCC will train six Master Trainers, who will in turn participate in training 22 healthcare professionals in “See & Treat” and mentoring the new trainees on a monthly basis during screening CCC will also train 25 community health volunteers in cervical cancer prevention and engage 65 CCC-trained community health volunteers to educate 25,000 people in the community. Together, these newly trained healthcare providers will mitigate the current shortage of healthcare workers and increase awareness of cervical cancer prevention.

- Equipment Donation: CCC will donate thermocoagulation treatment devices to six facilities along with other related screening supplies, as Replacing cryotherapy devices with thermocoagulation devices will save significant costs and will reach more women. Cryotherapy functions on carbon dioxide gas, which is expensive and often unavailable. Frequent shortages in the supply chain have forced women to wait or go elsewhere for treatment. Thermocoagulation is done with a handheld portable device that functions on rechargeable battery and can be used in any setting.
- Community Education: The 25 trained community health volunteers will conduct awareness talks in the community, advertise the “See & Treat” services, and assist with patient tracking and
- Strengthening Referral Chain: A key issue in decreasing the incidence of cervical cancer is the referral Women must have access to advanced diagnosis and care. CCC will work with stakeholders, including local/national government, to reach a 100 percent referral success rate from all 11 facilities. The expectation is that “See & Treat” will increase by 25 percent through community health volunteer referrals. This will turn a dysfunctional referral and follow-up system into an effective, closed-loop referral chain and feedback system.
- Monitoring and Evaluation: The Community Health Nurse will manage all aspects of the project, serve as the link between all stakeholders, perform regular site evaluation visits, and compile and send monthly data reports to
- Collaboration: CCC’s model is to partner with locally based and managed NGOs. KMET (Kisumu Medical Education and Trust) is CCC’s key ground partner for this project. KMET is an indigenous, Kisumu-based NGO established to promote quality health and education services across KMET will manage the Community Health Nurse (CHN) whose role is to manage the “See & Treat” project of the 11 health facilities and the mobile clinic.

- Community Health Nurse (CHN): The CHN is responsible for coordinating all aspects of the project – including monitoring/evaluating trainees, data management, tracking referrals, and coordinating screening events (in-reaches/outreaches). She coordinates the mentorship program with the Master Trainers for new trainees, tracks the impact of the community health volunteers while continuing to provide training, and holds monthly/quarterly meetings with various stakeholders, including organizations, government leadership, and healthcare She serves as the link between the facilities and the county government – advocating for the unique needs of the sites and supporting data collection at site level and delivery to county level. Most importantly, the CHN is the main contact for CCC, and participates in bi-weekly SKYPE calls and regular communication through email and Whatsapp.
- Measurement and evaluation: The Community Health Nurse will send monthly data reports from each of the 11 facilities and the mobile clinic indicating number of women screened, treated, referred, Her reports will also include how many men/women were educated by community health volunteers and how many women were referred to clinic by community health volunteers.
CCC has collected monthly data reports from every “See & Treat” site since inception. Based on experience with previous clinics, they have changed their model to include the Community Health Nurse to provide direct oversight and support for 1-5 years until the program can be absorbed and managed by hospital and local/national government. Additionally, CCC now provides financial support to the sites for 1-5 years until operational independence can be achieved.
 Recruitment for the various roles will be based on several factors. The Global Trainees (healthcare professionals) are invited to participate in training based on their current role and responsibilities at the facility, recommendation from senior leadership, and personal interest in offering “See & Treat.” Master Trainers will be selected based on demonstrated leadership skills, expertise in “See & Treat,” and personal interest in mentoring Global Trainees. The Community Health Volunteers will be chosen based on personal interest and proven track record of community engagement. Finally, patients are recruited from current outpatient programs such as HIV or family planning services as well as the mobile clinic, awareness talks, and one-on-one engagements with Community Health Volunteers.
Recruitment for the various roles will be based on several factors. The Global Trainees (healthcare professionals) are invited to participate in training based on their current role and responsibilities at the facility, recommendation from senior leadership, and personal interest in offering “See & Treat.” Master Trainers will be selected based on demonstrated leadership skills, expertise in “See & Treat,” and personal interest in mentoring Global Trainees. The Community Health Volunteers will be chosen based on personal interest and proven track record of community engagement. Finally, patients are recruited from current outpatient programs such as HIV or family planning services as well as the mobile clinic, awareness talks, and one-on-one engagements with Community Health Volunteers.
CCC plans to continue the partnership with KMET and Kisumu County for several years to achieve a Kisumu County-owned, led, and self-sustained organized screening program in public/private facilities. The long-term impact will be to decrease the incidence of cervical cancer in Kisumu County.
Impact: Direct Impact: 12,160; Indirect Impact: 25,000
UN Sustainable Development Goals
![]()
![]()
![]()
Questions for Discussion
- Why do you think it is important that men receive an education in cervical cancer screening?
- What do you expect would be the profile of the Community Health Nurse?
- How do you think this project might lead to preventative care in other areas of healthcare?
How the Grant Will be Used
NOTE: During these unprecedented times of COVID-19, Dining for Women has adapted grant funding and offered flexibility to grantees in the timeline, budgets and execution of their projects. These adjustments will be reported in the grantee reports.
DFW’s grant of $48,660.69 will be used for the following:
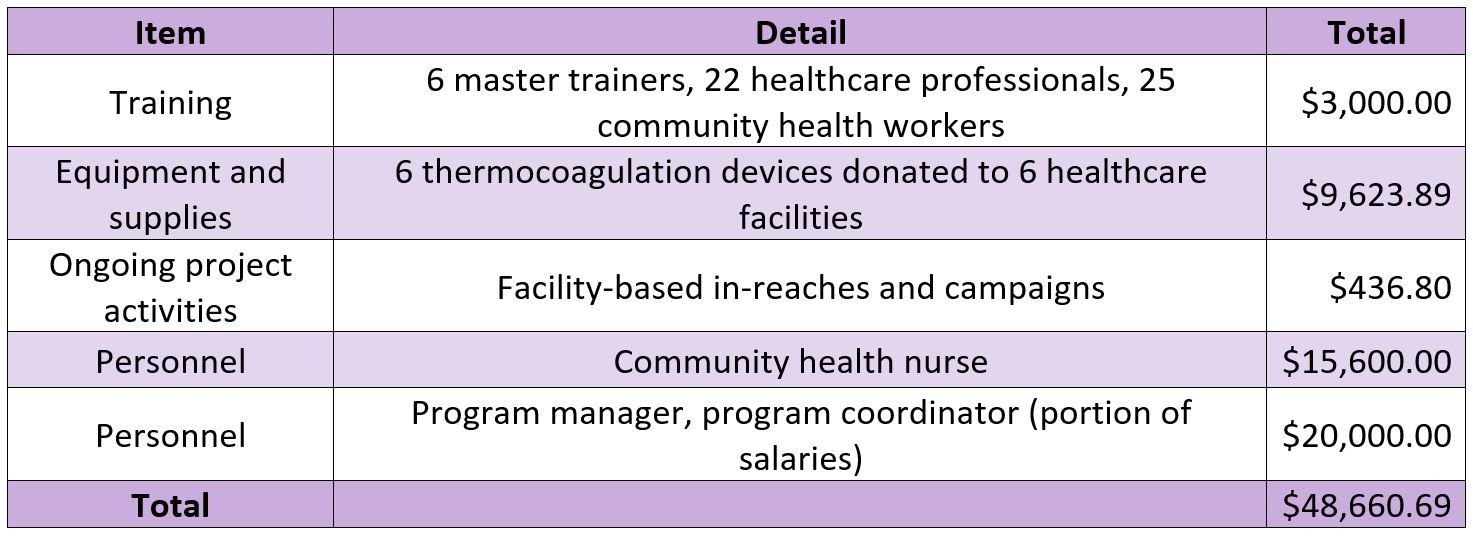
Why We Love This Project/Organization
We love CureCervicalCancer’s model of partnering with locally based nonprofits to save lives by preventing cervical cancer through early detection and treatment.
Evidence of Success
CCC has screened 114,630 women and treated 7,709 women for pre-cancerous lesions. This can also be interpreted as 7,709 lives saved. CCC has trained 600 healthcare professionals, trained 100+ community health volunteers, and established 90 sustainable “See & Treat” clinics. CCC has been honored with numerous awards:
- Joseph Drown Foundation Grant (2013, 2014, 2015, 2016)
- Ahmanson Foundation Grant (2014, 2015)
- Annenberg Foundation Grant (2015)
- Elizabeth Taylor AIDS Foundation Grant (2016)
- International Medical Corps Grant (2015, 2016)
- Distinguished Alumni Award (Dr. Patricia Gordon)
About the Organization
 CCC originated in 2012 after Dr. Patricia Gordon, a radiation oncologist, traveled to Dakar, Senegal, to treat women with cervical cancer. When the delayed arrival of the radiation machine necessitated changing plans, she organized a team of oncologists to provide screening and treatment services instead. Inspired by the life-saving impact of the simple and cost-effective VIA and ablation procedure (also called “See & Treat”), Dr. Gordon went on to establish CCC as a 501(c)3 nonprofit.
CCC originated in 2012 after Dr. Patricia Gordon, a radiation oncologist, traveled to Dakar, Senegal, to treat women with cervical cancer. When the delayed arrival of the radiation machine necessitated changing plans, she organized a team of oncologists to provide screening and treatment services instead. Inspired by the life-saving impact of the simple and cost-effective VIA and ablation procedure (also called “See & Treat”), Dr. Gordon went on to establish CCC as a 501(c)3 nonprofit.
CCC’s model creates sustainable screening and treatment clinics that serve thousands of women. They train healthcare professionals in the “See & Treat” method and partner with healthcare facilities to offer quality screening and treatment services, community-based outreach and education, and referral and follow-up linkages. CCC aims to achieve long-term sustainability by building local capacity.
CCC builds sustainable and community-driven programs by leveraging the resources and expertise of ground partners, including national and local organizations and governments. Through these partnerships, they build informed relationships with the community and with government officials as well as contract staff to provide project management. Some of CCC’s previous and current ground partners include International Medical Corps, Columbia Millennials Initiative, Innovating Health International, KMET, LVCT, Women4Cancer, and Syrian American Medical Society (SAMS). Additionally, CCC strategically partners with other like-minded groups to increase awareness, share resources, influence policy, and maximize impact.
The key activities and services CCC provide are:
 Training for Healthcare Professionals – CCC conducts intensive “See & Treat” trainings for healthcare professionals. CCC implements a train-the-trainer model by utilizing highly qualified local healthcare professionals to serve as facilitators during training and as mentors throughout the duration of the project. CCC continues to support the healthcare professionals by providing on-the-job training and formal refresher trainings.
Training for Healthcare Professionals – CCC conducts intensive “See & Treat” trainings for healthcare professionals. CCC implements a train-the-trainer model by utilizing highly qualified local healthcare professionals to serve as facilitators during training and as mentors throughout the duration of the project. CCC continues to support the healthcare professionals by providing on-the-job training and formal refresher trainings.
Community Health Volunteer Training – CCC trains and engages Community Health Volunteers as the vital link between the community and the clinic to increase patient volume, identify and track high risk patients, and conduct educational talks in the community setting. In settings where preventative care is not valued, Community Health Volunteers create demand by spreading awareness of the life-saving value of screening.
Donation of “Clinic in a Suitcase” – The largest costs for a “See & Treat” program are the initial expenses of equipment such as the thermocoagulation system to treat pre-cancerous lesions. CCC provides this equipment along with the necessary consumable supplies (speculums, gloves, acetic acid, bleach, etc.) until the clinic can operate independently.
Establishing Sustainable “See & Treat” Clinics and Mobile Clinics – With trained providers, equipment, and ongoing supervision and support, facilities can offer ongoing “See & Treat” services. Mobile clinics bring “See & Treat” to women who otherwise do not have access due distance or limited resources.
Technical Support for Cervical Cancer Prevention Program – In collaboration with local and national ground partners and government, CCC supports implementation of cervical cancer prevention through advocacy, service delivery, and community-based outreach/education.
Where They Work

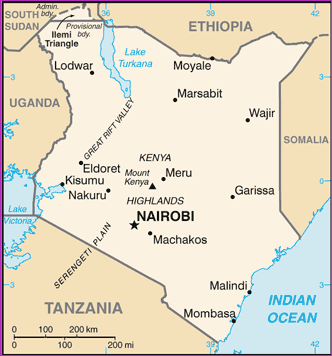
CCC has operated in 9 different countries since inception in 2012. Currently, CCC prioritizes projects in Kenya, Haiti, Tanzania, and Vietnam.
Kenya is in eastern Africa, bordering Somalia, Tanzania, South Sudan, Uganda, Ethiopia, and the Indian Ocean. It is twice the size of Nevada and home to just under 50 million people. The official languages are English and Kishwahili, although numerous indigenous languages are spoken. The climate varies from tropical along the coast to dry in the interior. There is recurring drought and flooding during the rainy season.
Kenya’s population has exploded since the mid-1900s due to its high birth rate, declining mortality rate, unmet need for family planning, and early marriage and childbearing. In the 90s, the government decreased emphasis on family planning to focus on the HIV epidemic instead. This combination of factors has resulted in a young population, with 40 percent of Kenyans under age 15. The rapid growth in population takes a toll on the labor market, social services, arable land, and natural resources.
Kenya is also a host country for refugees, as well as a source of emigrants. In the 60s and 70s, Kenyans emigrated to the US, UK, Soviet Union, and Canada to for study opportunities. In the 80s and 90s, Kenya experienced economic and political problems that resulted in a further outpouring of Kenyan students and professionals who sought opportunities in the west and in southern Africa. Conversely, Kenya has become home to hundreds of thousands of refugees since it gained independence in 1963. These refugees are typically fleeing violence in nearby countries. For instance, there are over 300,000 Somali refugees in Kenya.
Nairobi is the capital and largest city in Kenya, home to 3.3 million people and one of the largest cities in Africa. It lies in the southwest of the country in the highlands, at an elevation of 5,500 feet. Nairobi is home to thousands of businesses and over 100 major international companies and organizations. The city came to life in the late 1890s as a colonial railway settlement. While it is often mentioned as a jumping off point for safari-going foreigners, Nairobi is Kenya’s principal industrial center. Tourism is important, but its railways are the largest industrial employer, plus light manufacturing of beverages, cigarettes, and processed food.
 A closer look at how thermocoagulation is a new way of doing “See & Treat” for cervical cancer
A closer look at how thermocoagulation is a new way of doing “See & Treat” for cervical cancer
Cervical cancer is a leading cause of cancer-related deaths around the world, despite being highly preventable. Ninety percent of deaths caused by cervical cancer occur in developing regions where access to medical care is limited.
Unlike cryotherapy, which use cold temperatures to destroy pre-cancerous tissue, thermal coagulation uses heat. It is a simple 20 to 40 second procedure that only requires a reusable lightweight device that is electrically heated to approximately 100 degrees Celsius. It is typically performed by nurses and a variety of healthcare personnel, without anesthesia. Because it is effective, easily taught, and significantly less expensive than cryotherapy, thermal coagulation is a valuable tool against the ravages of cervical cancer in developing nations.
Source Materials
https://www.cia.gov/library/publications/the-world-factbook/geos/ke.html
https://www.britannica.com/place/Nairobi
https://www.ncbi.nlm.nih.gov/pubmed/30569837
https://www.who.int/publications-detail/guidelines-use-of-thermal-ablation-for-cervical-pre-cancer-lesions
https://www.thermo-coagulation.com/
https://www.medscape.com/viewarticle/910614