
Mission
TERREWODE’s mission is to build community capacity to eliminate obstetric fistula and systematically empower women and girls to meaningfully participate in the development process.
Life Challenges of the Women Served
 Obstetric fistula is a debilitating childbirth injury that results in uncontrollable incontinence of urine and/or feces that is caused by prolonged, obstructed labor and delayed access to quality emergency obstetric care. In many cases, the fetus dies during the prolonged labor, resulting in a double tragedy for these women. The social consequences of obstetric fistula are also extreme, as the odor from the incontinence leads to discrimination, stigma, shaming, social isolation, high rates of divorce and abandonment, and higher rates of gender-based violence (GBV). Economically, women with fistula are pushed deeper into poverty as they experience workforce discrimination and increased costs in health and hygiene needs. These women experience discrimination, loneliness, anger, low self-esteem, bitterness, depression, and suicidal thoughts.
Obstetric fistula is a debilitating childbirth injury that results in uncontrollable incontinence of urine and/or feces that is caused by prolonged, obstructed labor and delayed access to quality emergency obstetric care. In many cases, the fetus dies during the prolonged labor, resulting in a double tragedy for these women. The social consequences of obstetric fistula are also extreme, as the odor from the incontinence leads to discrimination, stigma, shaming, social isolation, high rates of divorce and abandonment, and higher rates of gender-based violence (GBV). Economically, women with fistula are pushed deeper into poverty as they experience workforce discrimination and increased costs in health and hygiene needs. These women experience discrimination, loneliness, anger, low self-esteem, bitterness, depression, and suicidal thoughts.
Uganda has one of the highest rates of obstetric fistula in the world. Estimates indicate as many as 140,000 – 200,000 women currently suffer from fistula and 1,900 new cases are added annually, though exact prevalence is difficult to measure. The capacity to treat fistula in Uganda, while improving, is only 2,400 women per year, resulting in a huge backlog of cases. Women who do receive treatment often wait months to years to access this care.
Obstetric fistula is most common among poor, rural, under-educated women with limited access to quality obstetric care. In Uganda, women in rural communities face significant socio-economic limitations characterized by high levels of household poverty, weak social service systems, and deeply rooted negative socio-cultural norms that aggravate gender disparities. As a result, rural women and girls have low decision-making power and limited access to and ownership of resources and skills required to access gainful employment.
Child marriage and early pregnancy in particular place girls and women at risk, as their young bodies are not fully developed, increasing the likelihood of obstructed labor. Young women and girls are also financially vulnerable and under-educated on their sexual and  reproductive health rights, thus when complications arise during labor, these women do not have the agency or economic means to advocate for the care they need. Sadly, Uganda also has the highest rate of teenage pregnancy in Sub-Saharan Africa: in 2016, nearly 25 percent of girls aged 15 – 19 were pregnant or had a baby.
reproductive health rights, thus when complications arise during labor, these women do not have the agency or economic means to advocate for the care they need. Sadly, Uganda also has the highest rate of teenage pregnancy in Sub-Saharan Africa: in 2016, nearly 25 percent of girls aged 15 – 19 were pregnant or had a baby.
Obstetric fistula is treatable and preventable, which is why it is rarely seen in high-income nations. Its prevalence is a clear indication that reproductive healthcare systems are failing to meet the needs of childbearing women. In Uganda, weak investment in rural health services has resulted in dire maternity care shortages, with long distances between health facilities that are understaffed and often lack essential drugs, supplies, and necessities such as gloves and electricity. Maternal mortality, commonly used as a proxy indicator for the overall strength of a health system, is also unacceptably high in Uganda, at 338 maternal deaths per 100,000 births. The chronically underfunded and under-provisioned health care system is plagued by a lack of infrastructure and equipment, essential drugs, and supplies.
Uganda also struggles with severe health worker shortages, with only nine physicians and 65 nurses or midwives per 100,000 people. Attraction and retention of health workers is difficult due to low salaries, poor benefits, and poor working conditions, including unsupportive supervision and underfunded and equipped health facilities Further compounding the problem is the severe maldistribution of the health workers – most of the health workforce is concentrated in urban areas, yet Uganda is predominantly rural; 84 percent of the population resides in rural areas. As a result, when rural women need emergency obstetric care, especially a caesarian delivery, they often experience long delays – sometimes days – before they receive the care they need. The high rate of obstetric fistula and maternal mortality can be directly attributed to these delays in receiving quality care.

Standard fistula treatment is predominantly focused on the surgical repair of the injury and two-week post-operative care during which medical staff may provide basic post-operative health education. With qualified surgical care, there is a high success rate in treatment, reported at 80 to 90 percent. Although women who receive surgical treatment for fistula often report increased quality of life and decreased rates of depression, many women report lingering psychosocial distress, ongoing depression, family discord, and economic difficulties even after successful treatment. In response, many fistula experts have called for fistula care that includes a comprehensive reintegration component to help women rebuild their lives post-repair. The World Health Organization’s recommendation for reintegration programs for fistula survivors includes in-depth psychosocial support, counseling, and economic empowerment. Unfortunately, this type of comprehensive care is not typically covered by local governments or foreign donor agencies and thus, treatment continues to focus solely on surgical care.
The effects of this trauma do not easily disappear after surgery. Women with supportive partners and families usually cope the best and, with time, can successfully reintegrate back into their community. However, women who experienced withdrawal of support, abandonment, and abuse, often struggle to reintegrate. This is more pronounced for extremely impoverished women and women who continue to experience physical co-morbidities from fistula, such as stress incontinence, secondary infertility, sexual disfunction, or pain. Young women and girls are particularly at-risk for ongoing reintegration difficulties. Almost half report ongoing health issues, a third desired additional personal or family counseling, and virtually all struggle economically.
TERREWODE has long recognized that surgery alone is not enough to heal from the trauma of an obstetric fistula and is concerned with the psychosocial, economic, and on-going health needs of women affected by this condition. Additionally, TERREWODE is concerned with increasing knowledge on safe motherhood and sexual and reproductive health rights to prevent the tragedy of fistula and improve maternal health overall.
The Project
TERREWODE’s Reintegration Program for Obstetric Fistula Survivors (RPOFS) addresses the lingering psycho-social, mental health, economic, and ongoing health needs of women who have suffered obstetric fistula. Women and girls gain health and sexual reproductive health knowledge, process and heal from psychological wounds, and gain practical income generating skills and financial literacy to rebuild their lives. Solidarity Groups and Music, Drama, and Dance groups provide ongoing support and mentorship, including financial support, to help lift women out of poverty. RPOFS aligns with the mission of Together Women Rise as it seeks to end extreme poverty for women and promote education and gender equality.
The primary beneficiaries are women and girls who have suffered from an obstetric fistula in Uganda. The program will be implemented in Soroti, Uganda, at the newly opened TERREWODE Women’s Community Hospital, with fistula survivors from eastern, central, and northern Uganda. The main goal is to provide the comprehensive care women need to fully heal from the trauma of fistula and successfully reintegrate into communities. The specific objectives of the Reintegration Program are to:
 improve mental health outcomes and family reunification/marital satisfaction among beneficiaries through the provision of psychosocial and family counseling,
improve mental health outcomes and family reunification/marital satisfaction among beneficiaries through the provision of psychosocial and family counseling,- improve beneficiaries’ long-term health outcomes and prevent fistula recurrence through the provision of education on obstetric fistula, safe motherhood, and family planning,
- improve the economic well-being of beneficiaries and their ability to meet their basic needs through the provision of microfinance, entrepreneurship, and income-generating skills training,
- create ongoing reintegration support networks for beneficiaries through the formation of Fistula Solidarity Groups and Music, Drama, and Dance groups, and
- increase beneficiaries’ awareness and understanding of their sexual reproductive health rights at local and national levels.
Expected outcomes include:
- 80 percent of participants will report improved mental health and self-esteem.
- All participants will understand the cause of fistula prevention.
- Zero fistula re-occurrence among participants.
- 75 percent of participants will engage in a micro savings group or for income generating activities (IGA).
- 75 percent of participants will join Fistula Solidarity or MDD groups, an indicator of ongoing reintegration support and empowerment.
- All participants will have increased awareness of their SRHR.
- Participants will engage in advocacy efforts for improved SRHR.
TERREWODE will achieve these outcomes by providing a holistic two-week Reintegration Program for Ugandan women who have suffered obstetric fistula. This will consist of psychosocial counseling (including family and marital counseling), health, nutrition, and safe motherhood education, family planning education and services, social reintegration support, and tools for economic empowerment. For many women, the health and safe motherhood education is the first time they truly understand why they experienced fistula. Critically, they also learn how to prevent fistula in future pregnancies.
 The program begins with a detailed needs assessment intake form, which allows TERREWODE to individualize specific aspects of the program to meet each woman’s needs. For example, some women may need marital counseling while others may need legal aid to establish their right to property after the breakup of their marriage. Intake needs assessments are conducted by one of TERREWODE’s trained fistula counselors. As women first tell their fistula story, this is also the beginning of their personal therapy. Each day entails individual components working with a fistula counselor and group classes. Women also have free time to bond with each other, sharing their stories with other women who understand the difficulties they have faced. For many women, this is the first time they have met other women suffering from fistula, and thus the first time they feel understood in their experience.
The program begins with a detailed needs assessment intake form, which allows TERREWODE to individualize specific aspects of the program to meet each woman’s needs. For example, some women may need marital counseling while others may need legal aid to establish their right to property after the breakup of their marriage. Intake needs assessments are conducted by one of TERREWODE’s trained fistula counselors. As women first tell their fistula story, this is also the beginning of their personal therapy. Each day entails individual components working with a fistula counselor and group classes. Women also have free time to bond with each other, sharing their stories with other women who understand the difficulties they have faced. For many women, this is the first time they have met other women suffering from fistula, and thus the first time they feel understood in their experience.
The economic components of the program include life skills, microfinance, and income-generating skills training with five different modules. Women learn about savings and business management and are encouraged to join savings groups when they return to their communities. Women are trained in different income generating activities based on their interest and community feasibility, which ensures the income generating activity will be successful and financially viable long-term. After graduating from the program, women have developed businesses in soap-making, beading, jewelry, tailoring, baking, mechanics, and hairdressing, among others.
Finally, the Reintegration Program provides training in human, legal, and sexual and reproductive health rights. TERREWODE staff equip women and girls affected by fistula with the tools and knowledge to enable women to advocate for their rights and to share their knowledge with their community.
A fundamental component of TERREWODE’s Reintegration Program stems from the understanding that social reintegration is a process and that therefore the women will require support after the two-week intensive program. To support this process, TERREWODE facilitates the formation of Solidarity Groups. Composed of fistula survivors, women’s group leaders, and community members, Solidarity Groups provide critical ongoing support, co-counseling, and self-reliance skills for women. Solidarity Groups serve as referral points for women with obstetric fistula or childbirth injuries. Group leaders refer women suspected of suffering from fistula to TERREWODE for treatment, and assist with reintegration post-treatment. Solidarity Groups also serve the wider community need by providing safe motherhood and SRHR education and advocacy, and women-to-women support systems. Many groups form micro-savings groups and assist one another with business strategies. TERREWODE staff provide field support visits to all Solidarity Groups.

Another innovative component of the program is TERREWODE’s Music, Drama, and Dance (MDD) program. During training, women use music, drama, and dance as part of their healing journey. Later, women have the option to join MDD groups and perform for local secondary schools, community groups, and during advocacy events, such as the International Day to End Fistula. MDD is a powerful, culturally resonate method to deliver messages about fistula awareness, ending child-marriage and GBV, among others. MDD provides an ongoing support network for women as well as a source of income. MDD groups are also open to male community members, and provide an opportunity for participation and training of men in SRHR and as allies in the movement.
The Reintegration Program will take place at TERREWODE Women’s Community Hospital (TWCH). The newly opened hospital includes a dedicated Reintegration Ward specifically constructed to accommodate the needs of this program. Transportation, meals and upkeep, supplies and family planning are all provided free of cost. Additionally, TWCH can offer the first physical therapy program for fistula and uterine injuries in the country, helping women heal from lingering co-morbidities of fistula.
 As a result of participating in the Reintegration Program, women will understand what caused their fistula and how they can protect themselves during future pregnancies. Psychosocial counseling will lead to decreased levels of depression, greater acceptance and forgiveness for the trauma they have endured, improved self-esteem and positive outlook. Participants will be ready to move forward and re-engage with life. Family counseling will lead to family reunification in most instances, though at times it is best for women to protect themselves from abusive family members. Women will gain skills and knowledge to earn an income and lift themselves out of poverty, and will join groups for on-going support and encouragement.
As a result of participating in the Reintegration Program, women will understand what caused their fistula and how they can protect themselves during future pregnancies. Psychosocial counseling will lead to decreased levels of depression, greater acceptance and forgiveness for the trauma they have endured, improved self-esteem and positive outlook. Participants will be ready to move forward and re-engage with life. Family counseling will lead to family reunification in most instances, though at times it is best for women to protect themselves from abusive family members. Women will gain skills and knowledge to earn an income and lift themselves out of poverty, and will join groups for on-going support and encouragement.
400 direct beneficiaries – Of these women and girls, approximately 300 will have received treatment at TERREWODE Women’s Community Hospital, and an additional 100 will be recruited after receiving care at government hospitals in Uganda. The women recruited from government hospitals will be selected based on need and vulnerability. The majority live in extreme poverty and earn less than $1.90 per day. Most are under-educated young women and girls: 60 percent are under the age of 24 when they suffer fistula, 65 percent suffered fistula with their first pregnancy, and less than 10 percent finished secondary education.
1,000 indirect beneficiaries – Also extremely impoverished, under-educated, and live in communities with poor social services and underfunded and dilapidated health infrastructure. They are primarily the family members of the 400 women who will attend the Reintegration Program. When indicated, couples and family counseling will be provided, with a goal of fostering family reunification when circumstances permit. Families will also benefit as women gain income generating skills and the skills and knowledge needed for successful business and savings ventures.
UN Sustainable Development Goals
![]()
![]()
Questions for Discussion
- How do society’s attitudes toward women affect the health care available to women?
- Why do you think child marriage persists and is even increasing during time of pandemic?
- Why do you think obstetric fistula in considered a solvable scourge?
- Why is it critical that support extend beyond the two-week program?
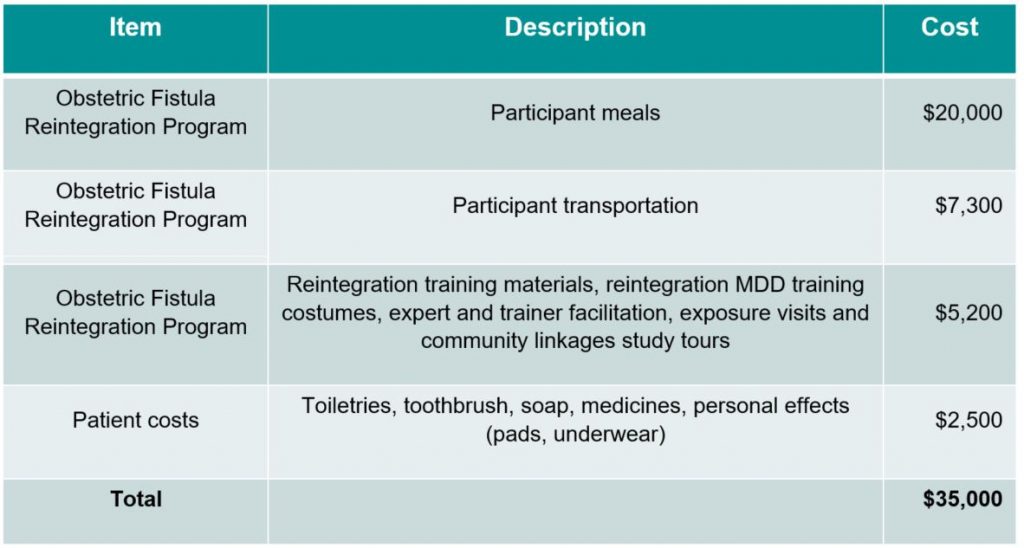
How the Grant Will be Used
Together Women Rise’s grant of $35,000 will fund:
Why We Love This Project/Organization
TERREWODE’s most valuable contribution to Ugandan women who have suffered obstetric fistula is to address the social consequences of obstetric fistula: the discrimination, stigma, shaming, social isolation, high rates of divorce and abandonment. Economically, women with fistula are pushed deeper into poverty as they experience workforce discrimination and increased costs in health and hygiene needs. The reintegration program that follows surgical repair allows new beginnings, a restoration of dignity and purpose, confidence and leadership. Educating the community on the risk factors for obstetric fistula is gradually creating cultural shifts and improving overall maternal health in Uganda.
Evidence of Success
TERREWODE is licensed by the National Non-Governmental Board, National Registration Bureau, and the Uganda Ministry of Health. Alice Emasu, the Executive Director of TERREWODE, was awarded the Golden Jubilee medal this year at Uganda’s International Women’s Day celebration for her groundbreaking work to improve maternal health and advocate for gender equality. Alice is also an Ashoka Fellow.
TERREWODE was a pioneer in underst anding the complex reintegration needs of women and developed its model Reintegration Program as a direct response to those needs. Since its founding, TERREWODE has supported treatment and reintegration services to more than 5,000 women and girls suffering from fistula. It has also supported (through training, advocacy, and education programs) over 2,000 community members, 27 Solidarity Groups with 800 members, and 39 women’s community groups. Additionally, more than 1,500 men have been trained in fistula awareness. Many of these men actively engage with TERREWODE in efforts to end fistula. TERREWODE has also been successful in bringing national attention to obstetric fistula using media, advocacy efforts, and partnership with the Ugandan Ministry of Health. This attention has led to greater awareness of the risks of fistula, increased demand for treatment from women suffering from fistula, and an increase in resources devoted to ending obstetric fistula.
 After 19 years, TERREWODE’s obstetric fistula program has been thoroughly tested, improved upon, and proven effective and sustainable. With the construction of TWCH, TERREWODE’s program has become much more robust, as high-quality routine fistula treatment and reintegration programming can be offered on site.
After 19 years, TERREWODE’s obstetric fistula program has been thoroughly tested, improved upon, and proven effective and sustainable. With the construction of TWCH, TERREWODE’s program has become much more robust, as high-quality routine fistula treatment and reintegration programming can be offered on site.
In addition to TERREWODE’s targeted prevention programs, many of the programs positively contribute to prevention. For example, the Reintegration Program creates economic opportunities for fistula survivors, and thus decreases their poverty and vulnerability to fistula reoccurrence. The Awareness and Advocacy Program educates women on their sexual and reproductive health rights and galvanizes efforts to improve maternal healthcare provision locally and nationwide.
TERREWODE has also recently established a research program with a dynamic agenda designed to examine the needs of women with fistula, test and improve its programs, and examine treatment and reintegration outcomes. The goal is to move the field of knowledge on fistula forward and to improve long-term outcomes and prevention strategies.
In 2013, beloved Ugandan musician Juliana Kanyomozi partnered with TERREWODE to produce a powerful song about obstetric fistula.
Voices of the Girls
“My relationship with TERREWODE has helped me a lot to live up to this time. One, the counseling I got from TERREWODE has helped me to understand myself and accept myself the way I am now. Secondly, it has given me that chance to join the group. Right now, I am in the number seven Solidarity Group. When I don’t have anything, I go to the group and borrow money from there. Up to now, if it was not for TERREWODE, I don’t know how I would have managed.”
– Woman with incurable fistula
“What helped me a lot was the counseling. TERREWODE taught me not to worry a lot about my life. That alone helped me because I have accepted myself. It helped me a lot.”
– Woman successfully treated
“My husband got counseling. I also personally counseled him because I got training from TERREWODE – there was a lot of counseling and advice. So when I went back home, I shared with him. And he accepted. And that’s why he’s now with me.”
– Woman successfully treated
“I tell you for me it is TERREWODE that helped. The business that I am doing, we were trained by TERREWODE. They told us that we can also still do something, we are still important. This business, the one that I’m doing, it is the result of the training that I started doing this – because I used to do nothing. But now I’m able to go out to the marketplace and take care of myself.”
– Woman with residual incontinence after repair
 Here women describe their experience living with fistula (excerpts from TERREWODE research 2017-2018):
Here women describe their experience living with fistula (excerpts from TERREWODE research 2017-2018):
“After fistula, my husband, who was responsible for the pregnancy, disliked me and took another wife. He told me he could no longer stay with a woman who’s so stenchy like me. I lost all hope and the only thing I could do was cry and cry. My relatives now all hated me, they said they could not even sit in my home.”
“Life with fistula is too hard. I wanted to socialize with people, but whenever I went near a group of people, some of them openly laughed at me. Others just marched away as soon as I reached the group. It was a really hard time for me.”
“The conditions at home are not good at all, I’m like a burden to my parents. They are fed up with me, they always complain about the smell, I’m like a problem, so I don’t feel comfortable at home. One time I thought about running away from home and just move. I also thought about killing myself.”
About the Organization
The Association for Rehabilitation and Re-orientation of Women for Development (TERREWODE) is a Uganda-based non-governmental organization founded in 1999 by Alice Emasu and two grassroot women leaders in Soroti District of eastern Uganda. TERREWODE was the first to break the silence that surrounded obstetric fistula in Uganda, bringing national attention and resources to address the issue. Today, TERREWODE is among the leading partners of the Ugandan Ministry of Health (MoH) in the national “End Fistula Campaign.” Alice Emasu, Executive Director, sits on the MoH National Obstetric Fistula Technical Working Group, assisting in producing obstetric fistula and maternal health strategies. TERREWODE has no religious affiliation and welcomes women of all backgrounds and beliefs.
Notably, there are no other organizations providing a comprehensive reintegration program for fistula survivors in TERREWODE’s service area, or in all of Uganda.
To secure treatment for women suffering from fistula, TERREWODE has worked for years within the existing medical system by securing grant funds for fistula treatment within government hospitals. However, over time TERREWODE found it was limited in its ability to effectively address critical needs of women and girls affected by obstetric fistula in government hospitals. TERREWODE found its model of providing holistic care was compromised by the inconsistent availability of quality treatment at government hospitals and we were frequently unhappy with the clinical outcomes of the women we brought there for treatment.
This led TERREWODE to develop a strategy of building its own facility where it can control the quality of care, achieve improved clinical outcomes, and increase the number of women treated annually. In 2014, TERREWODE began planning for the new hospital, secured a 6-acre plot of land, and raised funds towards the capital campaign with the assistance of its US partner, TERREWODE Women’s Fund. Construction on TERREWODE Women’s Community Hospital (TWCH) began in March 2018 and was completed in April 2019. Patient treatment began in August 2019. TWCH is the first and only dedicated fistula treatment hospital in Uganda and one of three in all of Africa.
 TERREWODE Women’s Fund (TWF), a US nonprofit organization, was founded in 2014. While TERREWODE has received support from nonprofit organizations over the years, TWF is dedicated solely to supporting TERREWODE’s mission and work. TWF was instrumental in helping to secure the land for the hospital and raise capital funds. TWF continues to fundraise for TERREWODE’s programs.
TERREWODE Women’s Fund (TWF), a US nonprofit organization, was founded in 2014. While TERREWODE has received support from nonprofit organizations over the years, TWF is dedicated solely to supporting TERREWODE’s mission and work. TWF was instrumental in helping to secure the land for the hospital and raise capital funds. TWF continues to fundraise for TERREWODE’s programs.
There are four key components of TERREWODE’s obstetric fistula program:
Awareness and Advocacy: TERREWODE trains a vibrant grassroots network of outreach volunteers, the Obstetric Fistula Awareness and Advocacy Network (OFAAN), to work in community settings to conduct fistula awareness activities, and to identify and refer fistula patients to TERREWODE for treatment and reintegration. Volunteers include leaders of local women’s and community groups, retired community leaders (known as the Dignity Watch Leaders), and finally, fistula survivors who have received treatment, counseling, and reintegration assistance. OFAAN volunteers support women after treatment as they reintegrate back into their community and link them with community resources that support their reintegration and empowerment. OFFAN volunteers work alongside fistula survivors to spread awareness about the cause and prevention of obstetric fistula in their communities. Finally, all volunteers and fistula survivors are educated on their sexual and reproductive health rights (SRHR) and provided knowledge, tools, and mentoring to advocate for their rights.
Treatment: The TERREWODE Women’s Community Hospital (TWCH) will increase the number of women treated for obstetric fistula and related childbirth injuries by 600 per year, greatly increasing Uganda’s current treatment capacity. Women who receive treatment at TWCH benefit from expert surgical care delivered in a state-of-the-art facility. TWCH is also improving surgical success rates, as their patients receive holistic, patient-centered care, including optimal nutrition and the necessary rest post-surgery to allow healing to occur. Finally, TWCH provides quality follow-up care to patients, which is critically important in achieving long-term continence, yet has been underfunded and rarely provided in government facilities.
Reintegration: TERREWODE realizes that surgery alone is not enough to heal from the trauma of an obstetric fistula, and thus developed the model reintegration program.
Prevention & Research: TERREWODE’s program is also built with the understanding that prevention is better than a cure. Obstetric fistula prevention is built into many of TERREWODE’s programs, such as the Music, Drama and Dance program. TERREWODE also uses radio ads to communicate fistula awareness and safe motherhood messages to rural communities and engage in local advocacy — calling on policy makers, policy implementers and other community leaders to improve situations of vulnerable women and girls. TERREWODE has also implemented innovative school programs targeting high school youth on the dangers of child marriages and teenage pregnancies, which are major contributing causes of fistula and maternal deaths in Uganda. Finally, TERREWODE implemented the Safe Motherhood Kit project, which empowers nurses and midwives and encourages antenatal care and birth at health facilities – a critical element in preventing fistula.
Where They Work

TERREWODE is headquartered in Soroti Municipality, in eastern Uganda, and has a liaison office in Kampala. TERREWODE’s initial service area was Soroti and the surrounding Teso District. Recently, the organization has expanded to serve women in eastern, central and northern Uganda, along with Sudanese refugees resettled in Uganda.
Uganda is home to 43 million people and many ethnic groups. One out of four live in the urban areas, with the majority concentrated in the central and southern regions near Lake Victoria and Lake Albert. The official language is English, but numerous other languages are spoken. Forty-five percent are protestant, 39 percent Catholic, and 14 percent Muslim. The country has been a source of refugees and a host of refugees from neighboring areas.
Unfortunately, the Ugandan government is plagued by corruption and poor management. There is little interest in investing adequately in health, education, and economic opportunities. Seventy-two percent work in some aspect of agriculture. Primary exports include coffee and gold. It has one of the world’s youngest and fastest growing populations, with a fertility rate also among the world’s highest at 5.8 children per woman. Not surprisingly, there is a widespread unmet need for contraception, a lack of government support for family planning and culturally, a preference for large families. Women have babies young and continue to give birth in close succession, which leads to a high maternal mortality rate. Ugandan women are less educated than the men, participate less in paid employment, and often have no control over childbearing.
Uganda is a landlocked country with many lakes and rivers. Lake Victoria is the world’s largest tropical lake and the second largest freshwater lake. The climate is tropical, with rain most of the year and two dry seasons. It is prone to droughts, floods, earthquakes, landslides and hailstorms.
 A closer look at the psychosocial reintegration needed for women who have suffered, many for decades, with fistula.
A closer look at the psychosocial reintegration needed for women who have suffered, many for decades, with fistula.
Numerous Sub-Saharan studies debunk the assumption that, after fistula repair, women will automatically heal, be seen as clean and respected members of their communities and families, and instantly reintegrate back into society. In reality, the process of psychosocial reintegration varies greatly depending on many factors, including a woman’s history of living with fistula. Reintegration may be even more challenging for women who have lived with fistula for many years, and who may have used common coping mechanisms such as limiting drinking water, taking frequent baths, applying perfumes, isolating, and washing clothes in secret.
Even after fistula repair, some women worry where they will live and about not being accepted by their husbands. A study in Kenya showed that half feared their husbands wouldn’t accept them despite the fistula repair. All hoped to have children in the future, especially those with no children. In Tanzania, a study proved that familial and economic support was key to reintegration, with 60 percent claiming that work was the most important factor in helping them feel “normal” again. In Ghana, a study showed that reintegration is challenged by historical and cultural norms, which results in many women feeling they have to prove themselves worthy of acceptance. As a result, some try to hide signs of post-repair urinary incontinence. A study of Ethiopian women showed that although most women with successfully repaired fistulas felt great relief, many were constantly fearful of developing another fistula and some continued to experience psychological and physical problems.
For a woman to truly regain her dignity and be reintegrated fully into family and society, it is imperative that a holistic approach be made available to her. This starts with counseling and follow-up medical care in a comprehensive treatment center, plus training so that she can find income-generating opportunities. In an effort to help these women feel less alone and stigmatized, they should also have the opportunity to connect with other women affected by fistula. Government can also play a key role by upgrading facilities to perform fistula repair surgery and offering it free of charge – thus showing women and the broader community that it is a priority.
Like TERREWODE’s multi-dimensional program, it is only when these components are firmly in place that women who have suffered from obstetric fistula can lead productive lives – and enjoy the freedom that gender equality allows.
Source Materials
https://cdn1.sph.harvard.edu/wp-content/uploads/sites/2413/2014/05/CounselingObstetricFistula_FistulaCare_TrainMat_2012.pdf
https://link.springer.com/article/10.1186/s12978-019-0692-y
https://www.sciencedirect.com/science/article/abs/pii/S1701216316354068
https://www.tandfonline.com/doi/abs/10.1080/17441692.2010.551519
https://www.tandfonline.com/doi/abs/10.1080/13691058.2014.964320
https://journals.sagepub.com/doi/full/10.1177/2158244015621112
https://link.springer.com/article/10.1007/s00192-019-03896-y
https://www.nepjol.info/index.php/NJOG/article/view/21714
https://onlinelibrary.wiley.com/doi/full/10.1111/tmi.13178
https://www.sciencedirect.com/science/article/abs/pii/S0266613817302255
https://www.cia.gov/library/publications/resources/the-world-factbook/geos/ug.html