
Mission
Care 2 Communities (C2C) has created a new, innovative approach for community healthcare delivery in Haiti: a social enterprise model that delivers reliable, affordable, high-quality primary care through a network of clinics. This community-based model, developed in partnership with the Haitian Ministry of Health, aims to transform the lives of vulnerable people by providing high-quality curative care, promoting good health, and ensuring sustainable long-term access to care.
Life Challenges of the Women Served
 Haiti is the poorest nation in the Western Hemisphere, and health outcomes for pregnant women and newborns are the lowest in the region. Health and education systems are fractured in Haiti, as decades of political and economic crises continue. Government hospitals and clinics have insufficient resources to provide reliable care to a poor population, and well-intentioned but unsystematic volunteer and missionary clinics across the country create confusion in the health marketplace. It is, simply, a dangerous place to be pregnant. Only 49 percent of women in Haiti give birth with a skilled attendant and only 39 percent deliver in a health facility. There is a high reliance on traditional medicine and voodoo practice in some areas, and health-seeking behavior regarding family planning is not a cultural norm. The WHO estimates that 91 percent of Haitians live within 5 kilometers of a health facility but only 23 percent – including just 5 percent of the rural population – have access to high-quality primary care.
Haiti is the poorest nation in the Western Hemisphere, and health outcomes for pregnant women and newborns are the lowest in the region. Health and education systems are fractured in Haiti, as decades of political and economic crises continue. Government hospitals and clinics have insufficient resources to provide reliable care to a poor population, and well-intentioned but unsystematic volunteer and missionary clinics across the country create confusion in the health marketplace. It is, simply, a dangerous place to be pregnant. Only 49 percent of women in Haiti give birth with a skilled attendant and only 39 percent deliver in a health facility. There is a high reliance on traditional medicine and voodoo practice in some areas, and health-seeking behavior regarding family planning is not a cultural norm. The WHO estimates that 91 percent of Haitians live within 5 kilometers of a health facility but only 23 percent – including just 5 percent of the rural population – have access to high-quality primary care.
The average age of first intercourse among women in Haiti is 17.7 years, and 56 percent of women reported first intercourse before age 18. Thirteen percent of girls ages 15 – 19 are sexually active, 10 percent of whom are pregnant or have at least one child. The impact of early, unintended pregnancies in impoverished communities is severe, including maternal and neonatal mortality. Young girls and women struggle to support their children, are not financially secure, and lack sufficient nutritional knowledge to ensure the best outcomes for their children.
The Project
 This DFW grant will allow C2C to launch a new sexual and reproductive health (SRH) education program to reach young women who have not yet accessed C2C’s family planning or antenatal services. This program will provide them with the information and tools they need to prevent early, unwanted pregnancies and gain control of their reproductive health. A 20-week SRH education after-school program will be piloted, with 400+ girls enrolled over a 12-month period. The program will include a new curriculum on reproductive health information for girls ages 13 – 20 who have not yet been pregnant. Over the course of the 12-month project, C2C will survey and measure SRH health knowledge on key topics, provide comprehensive education, and access knowledge retention. This project also promotes local leadership for girls and women in Northern Haiti as C2C will train local nurses to serve as educators, role models, leaders, and trusted sources of information for the project participants. By preventing unwanted pregnancy, participants in the project will be able to stay in school and receive the education that they need to break the poverty cycle and explore better opportunities that can change their lives, and the lives of their families and communities.
This DFW grant will allow C2C to launch a new sexual and reproductive health (SRH) education program to reach young women who have not yet accessed C2C’s family planning or antenatal services. This program will provide them with the information and tools they need to prevent early, unwanted pregnancies and gain control of their reproductive health. A 20-week SRH education after-school program will be piloted, with 400+ girls enrolled over a 12-month period. The program will include a new curriculum on reproductive health information for girls ages 13 – 20 who have not yet been pregnant. Over the course of the 12-month project, C2C will survey and measure SRH health knowledge on key topics, provide comprehensive education, and access knowledge retention. This project also promotes local leadership for girls and women in Northern Haiti as C2C will train local nurses to serve as educators, role models, leaders, and trusted sources of information for the project participants. By preventing unwanted pregnancy, participants in the project will be able to stay in school and receive the education that they need to break the poverty cycle and explore better opportunities that can change their lives, and the lives of their families and communities.
To reach the goal of preventing early, unwanted pregnancies in C2C’s service area through the proposed SRH education program, the following activities will be implemented at six C2C clinics in Northern Haiti during the one-year grant period:
- –
 Education Sessions: C2C will develop and implement a 20-week curriculum on SRH and family planning (FP) in each of their six clinic communities (two groups per community). Participants will be recruited at schools and community meetings. Sessions will be held after school hours, once a week at each clinic (two different groups of approximately 20 girls at each clinic site). Topics will include human development, gender roles, risk taking, relationships, sexual health, pregnancy risks, HIV and other STIs, consent, myths and misconceptions, and family planning. Strategies will include presentations, discussions, videos, games, scenarios/role-play, and anonymous questions. Taught by a team of three nurses, the sessions will develop skills in communication, problem-solving, decision-making, condom negotiation and use, and behavior
Education Sessions: C2C will develop and implement a 20-week curriculum on SRH and family planning (FP) in each of their six clinic communities (two groups per community). Participants will be recruited at schools and community meetings. Sessions will be held after school hours, once a week at each clinic (two different groups of approximately 20 girls at each clinic site). Topics will include human development, gender roles, risk taking, relationships, sexual health, pregnancy risks, HIV and other STIs, consent, myths and misconceptions, and family planning. Strategies will include presentations, discussions, videos, games, scenarios/role-play, and anonymous questions. Taught by a team of three nurses, the sessions will develop skills in communication, problem-solving, decision-making, condom negotiation and use, and behavior - – Health Screenings and Counseling for Program Participants: These will include all necessary lab tests (vaginal smear, urine test, complete blood count, pregnancy test, gonorrhea and chlamydia tests, HIV, and syphilis tests). Each participant will receive a free health screening with a doctor at the beginning and at the end of the
- – Staff Training and Monitoring: The lack of quality healthcare in Haiti is a key factor in low health-seeking behaviors, low utilization of family planning, and low medication compliance rates. Young girls are not empowered to seek out family planning services and staff members are not trained to respond to young girls seeking FP. C2C will provide training to each of their staff members involved in FP decision-making (one auxiliary nurse and doctor per clinic, plus one midwife and OB/GYN) to better promote FP services to young girls. The staff will counsel girls in their decision-making process, better explain different FP methods and their potential side effects, invite questions, and follow-up with young girls using FP for the first time. C2C will create a brochure to assist in decision-making, create a script for staff to follow when addressing young girls that have never used FP, develop evaluation criteria, and evaluate staff
 members for quality of care.
members for quality of care. - – Free Family Planning Services and Commodities: C2C will offer FP services and commodities at all their clinics at no cost for those who complete the education program. The Haitian government subsidizes these commodities, but C2C will backstop the government to ensure a steady, reliable supply.
Participants will be recruited at schools and community meetings by C2C’s community health workers and nurses. (They regularly visit schools in each community to promote vaccination coverage and nutrition and will incorporate recruiting into those visits.) Any female ages 13 – 20 will be encouraged to attend, especially those who have never accessed FP services.
C2C’s research shows that approximately six individuals reside in an average Haitian household. By providing SRH education to girls ages 13 – 20 in 400 typical households, they will indirectly impact 2,400+ people in Northern Haiti whose households and families would be affected by a program participant’s early pregnancy. Of those indirectly impacted, they estimate that 50 percent will be women and girls.
Impact: Direct: 400; Indirect: 2,400
UN Sustainable Development Goals
![]()
![]()
Questions for Discussion
- How do you think sexual health awareness education can impact poverty and gender equality?
- Can learning about their sexual rights promote self-sufficiency for girls and women?
- What is the impact of limited access to healthcare services on women worldwide?
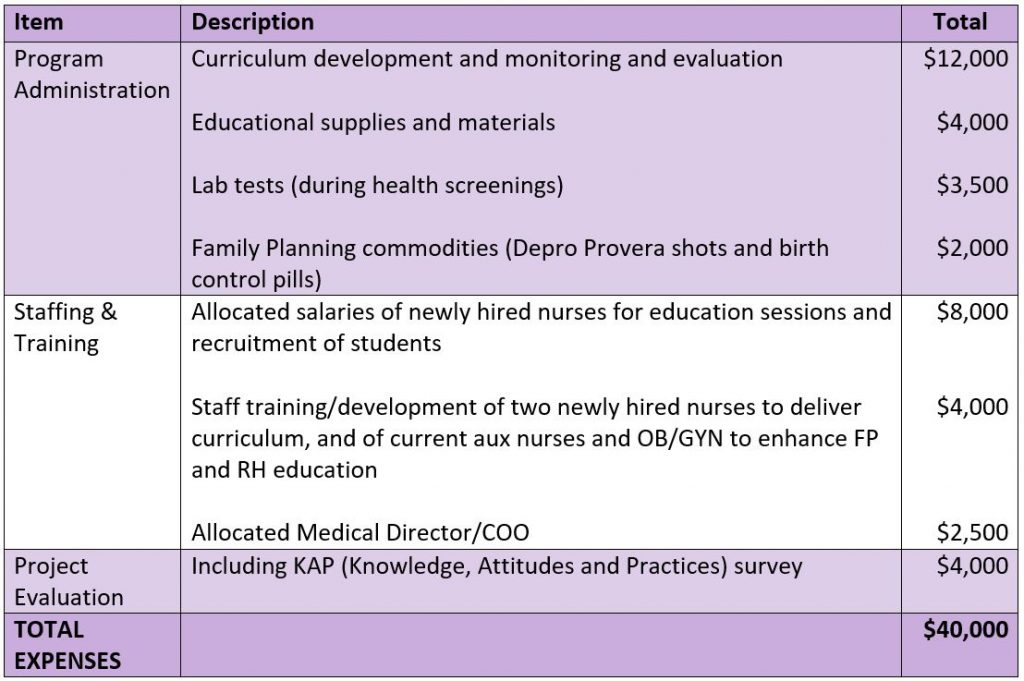
How the Grant Will be Used
DFW’s grant of $40,000 will be used for the following:
Why We Love This Project/Organization
Care 2 Communities uses a unique model of encouraging public/private partnerships to improve healthcare in isolated poor communities. By operating clinics as efficient, community-based businesses, C2C has proven that low-income people are willing and able to pay for health services that meet their needs, cure illnesses, and treat them respectfully. C2C seeks to increase knowledge and awareness of sexual reproductive health among young girls between the ages of 13-20 in a country with poor maternal outcomes. This allows for prudent decision-making and helps prevent the challenges of young teens delivering and raising children in poverty.
Evidence of Success
 C2C’s model is delivering positive change by improving access to high-quality healthcare at government clinics in Haiti. Their low user fees are recovering 75 – 90 percent of operating costs at each distinct clinic unit. In 2019, C2C clinics reached 30,000+ patients (up from 16,000 just two years prior) and they have agreements in place to launch/rehabilitate six additional public clinics in the next two years. At newly integrated public-private partnership clinics with the Ministry of Health, the Ministry’s aggregated health delivery quality score has risen by 40 percent pre/post C2C’s involvement; patient volume has increased by 50 percent (from an average of eight patients a day to 12 patients a day); lab capacity has increased by 66 percent (from an average of nine tests to 15 tests available); availability of pharmaceuticals has increased 300 percent (from average of 29 medications to 88 medications available), and prices on average have decreased 15 percent for labs and 25 percent for medications. C2C has also implemented a maternal health program at two clinics that have been successful at reaching vulnerable women with much needed antenatal and newborn care. In its first three years, they have treated approximately 2,500 unique pregnant women and conducted 9,125 consultative visits through their maternal health program. C2C’s Community Health Workers have conducted over 15,000 home visits to provide health education and clinical follow-up.
C2C’s model is delivering positive change by improving access to high-quality healthcare at government clinics in Haiti. Their low user fees are recovering 75 – 90 percent of operating costs at each distinct clinic unit. In 2019, C2C clinics reached 30,000+ patients (up from 16,000 just two years prior) and they have agreements in place to launch/rehabilitate six additional public clinics in the next two years. At newly integrated public-private partnership clinics with the Ministry of Health, the Ministry’s aggregated health delivery quality score has risen by 40 percent pre/post C2C’s involvement; patient volume has increased by 50 percent (from an average of eight patients a day to 12 patients a day); lab capacity has increased by 66 percent (from an average of nine tests to 15 tests available); availability of pharmaceuticals has increased 300 percent (from average of 29 medications to 88 medications available), and prices on average have decreased 15 percent for labs and 25 percent for medications. C2C has also implemented a maternal health program at two clinics that have been successful at reaching vulnerable women with much needed antenatal and newborn care. In its first three years, they have treated approximately 2,500 unique pregnant women and conducted 9,125 consultative visits through their maternal health program. C2C’s Community Health Workers have conducted over 15,000 home visits to provide health education and clinical follow-up.
Voices of the Girls
From C2C participants:
“One of the greatest gifts we have in having this clinic in the community is the dynamic staff that takes care of us.”
“We are very fortunate to have a maternal health clinic right in our community, many other communities wish they had that opportunity.”
 “I’m pregnant with my third child and with all my pregnancies I’ve consulted at C2C, which has been very convenient and affordable.”
“I’m pregnant with my third child and with all my pregnancies I’ve consulted at C2C, which has been very convenient and affordable.”
“I look forward to coming to my prenatal visit since I get to chat with other pregnant ladies and discuss our pregnancies.”
“I thank God that this clinic is here since I am having a complicated pregnancy and I get to see an OBGYN all through my pregnancy.”
“I am young, and this is my first pregnancy, and I am glad that there is a midwife at C2C where I can ask her all my questions and concerns. I feel at ease with her.”
“I have been coming to this clinic for the past four years for family planning and I thank God it will always be here for the community.”
About the Organization
C2C was founded in 2009 by Elizabeth Sheehan, a Physician’s Assistant and health economist who spent over a decade working in hospitals and clinics in Africa and East Asia. She witnessed firsthand the tragedy of people dying from treatable and preventable illness. She set out to create a high-quality community clinic model that she knew would change, and save, lives.
To ensure long-term financial sustainability of a community clinic network, Elizabeth and her team created an operating model with a social enterprise approach and a focus on primary care and maternal health. In 2018, C2C formed a public-private partnership (PPP) with the Haitian Ministry of Health and is currently scaling its successful model by “rehabilitating” and taking over the management at underperforming government clinics throughout Northern Haiti.
In the past two years, C2C has doubled its footprint, expanding from three to six clinics, and now serving 30,000+ patients annually, with plans to expand to three more government clinics in the next year. C2C is committed to primary care and has a focus on women’s health through their antenatal care and family planning services. Ensuring women have control over their reproductive health is an urgent priority for C2C. C2C has 55 employees (50 in Haiti) and a 13-member Board of Directors who bring expertise in business, finance, public health, medicine, and enterprise development.
Where They Work


Haiti is in the Caribbean on the western one-third of the island of Hispaniola, between the Caribbean Sea and North Atlantic Ocean, west of the Dominican Republic. It is currently the poorest country in the Western Hemisphere, with close to 60 percent of the population living below the national poverty line.
Its area is slightly smaller than the state of Maryland. The terrain is mostly rough and mountainous with 66.4 percent agricultural land. The population is distributed fairly evenly, with the largest concentrations located near coastal areas. Its population is 11,067,777 (July 2020 est.).
 The median age in Haiti is 24.1 years, and the life expectancy is 65.3 years. The birth rate is 21.7 births/1,000 population, with the mother’s mean age of first birth being 22.8 years. The maternal mortality rate is 480 deaths/100,000 live births, and the infant mortality rate is 42.6 deaths/1,000 live births. The percentage of underweight children under the age of 5 years is 9.5 percent. The literacy rate for women is 58.3 percent, and 65.3 percent for men.
The median age in Haiti is 24.1 years, and the life expectancy is 65.3 years. The birth rate is 21.7 births/1,000 population, with the mother’s mean age of first birth being 22.8 years. The maternal mortality rate is 480 deaths/100,000 live births, and the infant mortality rate is 42.6 deaths/1,000 live births. The percentage of underweight children under the age of 5 years is 9.5 percent. The literacy rate for women is 58.3 percent, and 65.3 percent for men.
Two-fifths of all Haitians depend on the agricultural sector, mainly small-scale subsistence farming, which remains vulnerable to damage from frequent natural disasters. Poverty, corruption, vulnerability to natural disasters, and low levels of education for much of the population represent some of the most serious impediments to Haiti’s economic growth
A Closer Look at Teen Sexual Health
For millions of young people around the world, the onset of adolescence brings not only changes to their bodies but also new vulnerabilities to human rights abuses, particularly in the arenas of sexuality, marriage, and childbearing.
Young people worldwide reach puberty earlier and marry later than in the past. As a result, youth are sexually mature for a long period of time prior to marriage. Premarital sexual intercourse is common and appears to be on the rise in all regions of the world. Studies of female youth suggest that that 2 – 11 percent of Asian women have had sexual intercourse by age 18; 12 – 44 percent of Latin American women by age 16; and 45 – 52 percent of sub-Saharan African women by age 19.3. In developed countries, most young women have had sex prior to age 20 – 67 percent in France, 79 percent in Great Britain, and 71 percent in the United States.
 One of the most common sexual relationships among young girls, especially those from the lower economic echelon, is sexual relations with older men from a better economic status who are commonly known as “sugar daddies” Transactional sex (TS) or sexual relations with “sugar daddies” is defined as heterosexual intercourse with a nonmarital partner 10 or more years older, primarily characterized by relationships between younger women and older men. To get material benefits, girls expose themselves to serious health risks.
One of the most common sexual relationships among young girls, especially those from the lower economic echelon, is sexual relations with older men from a better economic status who are commonly known as “sugar daddies” Transactional sex (TS) or sexual relations with “sugar daddies” is defined as heterosexual intercourse with a nonmarital partner 10 or more years older, primarily characterized by relationships between younger women and older men. To get material benefits, girls expose themselves to serious health risks.
Between 2011 and 2020, an estimated 140 million girls have become child brides, according to the United Nations Population Fund. If current levels of child marriages hold, 14.2 million girls annually or 39,000 daily will marry too young. Furthermore, of the 140 million girls who will marry before they are 18, 50 million will be under the age of 15.
Young people’s sexual activity is not always consensual. Some countries – such as Bangladesh, Brazil, and Thailand – report that many children are forced into prostitution. In the United States, studies suggest that about one-in-three young girls and one-in-six young boys may have experienced at least one sexually abusive episode before adulthood.
Millions of girls are coerced into unwanted sex or marriage, putting them at risk of unwanted pregnancies, unsafe abortions, sexually transmitted infections (STIs) including HIV, and dangerous childbirth. Adolescent boys are at risk, as well. Young people – both boys and girls – are disproportionately affected by HIV.
 Adolescent pregnancy and childbearing are associated with a range of outcomes detrimental to teens’ health, including complications of pregnancy. When compared to women in their mid-20s, women under age 15 are at 25 times greater risk of dying from complications related to pregnancy or childbirth; 15- to 19-year-old women are at twice the risk.
Adolescent pregnancy and childbearing are associated with a range of outcomes detrimental to teens’ health, including complications of pregnancy. When compared to women in their mid-20s, women under age 15 are at 25 times greater risk of dying from complications related to pregnancy or childbirth; 15- to 19-year-old women are at twice the risk.
Although rates of adolescent childbearing are declining in many countries, 15 million women ages 15 – 19 give birth every year, 13 million in less developed countries. Overall, 33 percent of women from less developed countries give birth before the age of 20 – varying from 8 percent in East Asia to 55 percent in West Africa. In developed countries, up to 10 percent of women give birth by age 20, except in the United States, where up to 19 percent give birth by age 20. Adolescent pregnancies are a global problem occurring in high-, middle-, and low-income countries.
Worldwide, mostly because of unintended pregnancy, nearly four and a half million adolescents undergo abortion each year; 40 percent of which occur under unsafe conditions. Adolescent pregnancy and childbearing often lead girls into dropping out of school, jeopardizing girls’ future education and employment opportunities.
Source Materials