
Childbirth continues to claim far too many lives
By Marcie Christensen and Donna Shaver
For many years, the accepted wisdom was that a woman died in childbirth somewhere in the world roughly every minute of every day, 365 days a year—for a total of 543,000 per year. The vast majority of those deaths occurred in sub-Saharan Africa and Southern Asia. Most were in rural areas, and among poor populations. In 2008, a study published in The Lancet reported that the number had dropped to 342,000. In May 2012, the World Health Organization (WHO), The United Nations Children’s Fund (UNICEF), the United Nations Population Fund (UNFPA), and the World Bank released a new study, showing that the number of maternal deaths had been nearly cut in half, dropping from 543,000 to 287,000 from 1990 – 2010.
Still, this means that every two minutes, a woman dies of pregnancy-related complications. There are five common causes:
- Severe bleeding after childbirth
- Infections
- Obstructed labor
- High blood pressure during pregnancy (pre-eclampsia)
- Unsafe abortion
Most important to note is that 99 percent of maternal deaths occur in developing countries, and most could have been prevented with appropriate interventions. Only half of women in these regions received recommended health care during pregnancy.
Primary obstacles to adequate maternal health care include:
- Lack of skilled birth attendants
- Difficulty of attracting and retaining skilled providers in remote locations
- Few clinics in rural areas, and those that exist are often understaffed
- Poor transportation infrastructure
- Need for midwives
- Problems with quality of care and treatment of birthing mothers
- Corruption
Bumi Sehat operates a clinic in Bali to provide access to quality healthcare and kind, hygienic, culturally appropriate childbirth. Bumi Sehat believes that each baby’s capacity to love and trust is built at birth and in the first two hours of life. By protecting pregnancy, birth, postpartum care and breastfeeding, the midwives at Bumi Sehat are advocating for optimal humanity, health, intelligence, and consciousness.
Indonesia’s maternal mortality rate is 220 per every 100,000 live births. Contrasted with Somalia (at 1,000) and Sierra Leone (nearly 900), Indonesia’s record seems admirable. However, with a country-wide goal of reducing maternal mortality to just over 100 per 100,000 live births by 2015, Indonesia is currently short of its goal.
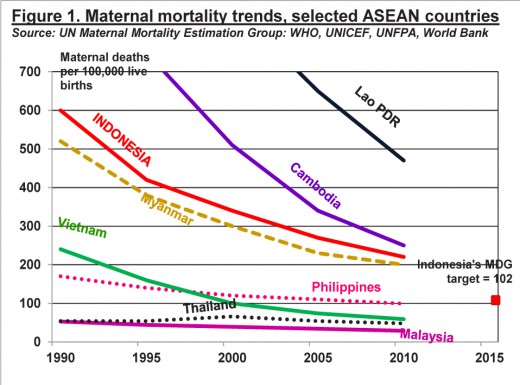
Indonesia’s progress on maternal health has slowed in recent years. Its maternal mortality ratio has remained above 200 over the past decade, despite efforts to improve maternal health services. The country’s 83 percent of births attended by a doctor, nurse, or midwife is a good indicator of progress, but only 63 percent of births take place in hospitals and clinics. Poorer countries in the region have shown greater progress in this regard.
Considerations in Maternal Health
- Child Marriage: Marriage before age 20 is a concern. A girl’s or young woman’s body is not prepared for childbirth. In developing countries, many girls are stunted (malnourished and underweight for their age) making them all the more likely to die in childbirth or suffer a serious childbirth injury. Girls younger than 15 are five times more likely to die in childbirth than women in their twenties. Pregnancy is the leading cause of death worldwide for women ages 15 to 19. In Indonesia, only three percent of girls are married before age 15, and only 17 percent before age 18.
- Childbirth injuries to mother: Obstetric fistula is a childbirth injury resulting from obstructed labor. When the baby cannot pass through the mother’s pelvis, the birth contractions continue to keep the head lodged against the bones of the pelvis. Without medical intervention, the baby usually dies, and the mother sustains damage to her birth canal that can only be reversed by surgery. (Learn more about fistula in Food for Thought – May 2014.)
- Complications during pregnancy and delivery: Pre-eclampsia is a complication of pregnancy. Women with pre-eclampsia have high blood pressure, protein in their urine, and may develop other symptoms and problems. The more severe pre-eclampsia is, the greater the risk of serious complications to both mother and baby. Women who have access to medical care throughout their pregnancies can be monitored and treated.
- Neonatal mortality: Mortality often resulting from pre-term birth, a variety of maternal health factors contribute, including adolescent pregnancy, HIV/AIDS infection. (Learn more about neonatal mortality in Food for Thought – July 2013.)
- Female Genital Mutilation (FGM): FGM affects more women in Sub-Saharan Africa than anywhere else in the world. The procedure results in scar tissue that can make birth difficult. A study done by the World Health Organization shows “evidence that deliveries among women who have been subject to FGM are significantly more likely to be complicated and dangerous.” The danger is to both mothers and babies. Mothers are more likely to hemorrhage. Babies are in substantial danger during birth, as they are far more likely to have to be resuscitated, having been deprived of oxygen during the difficult delivery. The death rate for babies was much higher for women who had undergone the procedure, with the danger increasing according to the level of FGM.
- Fertility and contraception: With each additional pregnancy, the odds of maternal mortality increase. The mother’s health may be compromised from hard work and poor nutrition. Many women would like to space their children, but lack access to contraception. In addition, women are responsible for a great deal of the physical labor—from carrying water to gathering firewood to building and maintaining the family’s shelter to farming. Pregnancy does not excuse a woman from her chores, as there is may be no one else to do them.
 Millennium Development Goals and Beyond 2015
Millennium Development Goals and Beyond 2015

- The maternal mortality ratio dropped by 45 percent between 1990 and 2013, from 380 to 210 deaths per 100,000 live births. All regions have made progress but accelerated interventions are required in order meet the target.
- In Eastern Asia, Northern Africa and Southern Asia, maternal mortality has declined by around two-thirds.
- The proportion of deliveries in developing regions attended by skilled health personnel rose from 56 in 1990 to 68 per cent in 2012.
- The maternal mortality ratio in developing regions is still 14 times higher than in the developed regions.
- The rural-urban gap in skilled care during childbirth has narrowed.
Target 5.B: Achieve, by 2015, universal access to reproductive health
- More women are receiving post-natal care. In developing regions, it increased from 65 percent in 1990 to 83 per cent in 2012.
- Only half of women in developing regions receive the recommended amount of health care they need.
- Fewer teens are having children in most developing regions, but progress has slowed.
- The large increase in contraceptive use in the 1990s was not matched in the 2000s.
- The need for family planning is slowly being met for more women, but demand is increasing at a rapid pace.
- Official Development Assistance for reproductive health care and family planning remains low.
Beyond 2015 is a global civil society campaign, pushing for a strong and legitimate successor framework to the Millennium Development Goals. The campaign, created in 2010, is built on a diverse, global base. It ranges from small community based organizations to international NGOs, academics and trade unions. A founding principle of the campaign is that it is a partnership between civil society organizations from the ‘North’ and the ‘South’ – bringing together groups from developing, emerging and developed economies.
The ‘Values and Targets’ document provides a list of 40 targets which cut across Beyond 2015’s values. These targets will be a key advocacy tool for the whole campaign throughout the intergovernmental negotiations around the post-2015 agenda. Target 34 is “Ensure universal access to quality health services, including sexual and reproductive healthcare and rights, and covering both communicable and non-communicable diseases.”
Beyond 2015 invites citizens, civil society, Member States and UN agencies to help refine these documents by sharing feedback online. If the online ‘satisfaction gauge’ falls below 50 percent, they will rewrite the documents. The current (9-1-2014) ‘satisfaction gauge’ is 49.5 percent.
This is your opportunity to contribute to the definition of our common positions going forward and of the lens through which Beyond 2015 assesses the High Level Panel’s and other UN actors’ reports and positions!
Recommended reading
Note: Each year’s UNICEF State of the World’s Children report highlights a different topic. Statistics in this Food for Thought are from the 2014 report.
- The State of the World’s Children 2009 – examines critical issues in maternal and newborn health, underscoring the need to establish a comprehensive continuum of care for mothers, newborns, and children
- The State of the World’s Children 2014 – highlights the critical role data and monitoring play in realizing children’s rights. Credible data, disseminated effectively and used correctly, make it possible to target interventions that help right the wrong of exclusion.